










Since 2005, HIV cases in Indonesia tend to increase every year. By the end of 2020, the cumulative number of people living with HIV/AIDS (PLWHA) was 419,551, spread throughout the nation (Indonesian Ministry of Health, 2021). The HIV prevalence was reported among many groups, such as drug users (4.3%), heterosexuals (30.8%), homosexuals (17.2%), prostitutes and their clients (68%) (Indonesian Ministry of Health, 2021). Therefore, it is indicated that HIV has already spread in the general community.
Of the total adult HIV infections, 33% are confirmed as women. It is estimated that the majority of them acquired the virus from their intimate partners. This condition indicates that many uninfected women have been living in serodiscordant relationships. In the area of HIV/AIDS, the term serodiscordant relationship is usually used to refer to a couple who engages in a relationship in which one partner is HIV-positive, and another partner is HIV-negative (World Health Organization, 2012). At the same time, uninfected women in serodiscordant relationships are extremely high risk of becoming infected. They also may be stigmatized by the community because of their partner’s HIV status.
HIV-related stigma is one of the biggest challenges for PLWHA and their families. HIV/AIDS-related stigma has been seen worldwide, even though it manifests differently between individuals, groups, cultures, and countries. UNAIDS reported that more than 50% of people aged 15 to 49 having discriminating attitudes towards people living with HIV (UNAIDS, 2020). People perceive HIV/AIDS as misbehaving and immoral behaviors, such as drug use, sex workers, homosexuals, and transgender people. The HIV/AIDS prevention programs, which mainly focus on the high-risk groups or key populations, may contribute to exacerbates HIV-related stigma. As a result, those beliefs caused negative social judgment and discrimination for everyone with HIV positive and their family.
The stigma experienced by PLWHA and their family comes from close friends, neighbors, colleagues in workplaces, and healthcare workers (Putri et al., 2019; Juanamasta et al., 2020). Experiences of stigma are prevalent and include being subjected to gossip, rumors, and name-calling, and HIV-negative partners being labeled HIV-positive (Rispel et al., 2015). Another study has categorized the form of stigma experienced by HIV-negative partners as distancing, depreciation, violation of privacy, and accusation (Siegel et al., 2018). Goffman (1963) proposed stigma that affects those closely associated with stigmatized individuals and the group as a courtesy stigma.
In Indonesia, HIV-related stigma was initially started by the first case found when a Dutch homosexual tourist died in Bali in 1987. This first case made the Indonesian community perceived HIV as a foreign disease. Afterward, new cases of HIV were added by female sex workers in 1991. The new cases lead people to view HIV as a foreign and homosexual disease and as a disease of female sex workers. The stigma toward the latter group becomes a challenge for women in Indonesia, either they are HIV positive or a wife to a husband with HIV positive. A wife in a negative serodiscordant relationship is stigmatized by their community as if they share the same disease with their husband (Imelda, 2011).
HIV-related stigma is more pronounced in Indonesia, as a predominantly Muslim country. It happens because of the religious beliefs, in which most of the ways of HIV transmission violate religious prohibitions such as same-sex practices, extramarital sex, adultery, and drug use (Hasnain, 2005). Muslim society considers HIV/AIDS as a moral-religious issue rather than a health problem. Most people believe that HIV/AIDS is a punishment from God for violating society and religion (Badahdah, 2010). Regardless of the violation of forbidden behavior as the cause of the husband’s HIV status, Muslim wives decided to continue their marriage (Agnes Yeni et al., 2020). The decision to stay in a serodiscordant relationship may cause psychological disruption among HIV-negative wives, such as anger toward their husbands since they knew their husbands’ HIV-positive status during their marriage. They also fear being infected and stigmatized (Larki, 2020). On the one hand, living in a serodiscordant relationship puts HIV-negative wives experienced courtesy stigma. On the other hand, their situation may lead them to be stigmatizers toward their husbands.
Numerous studies have explored HIV-related stigma and coping strategies among PLWHA. They faced HIV-related stigma by seeking social support, emotional support, practical support, and stigma-reducing interventions (Chambers et al., 2015; Anima-Korang et al., 2018). They also did selective disclosure to their family, friends, HIV activists, and health care providers as a positive coping strategy (Kumar et al., 2015; Mendelsohn et al., 2015). However, there is still a lack of explanation of the HIV-negative wives’ experiences disclosing their serodiscordant relationship. One qualitative study described that HIV-negative wives disclosed their husband’s HIV-positive status to a limited person to avoid negative experiences from family, friends, and health care providers (Larki, 2020). The fear of HIV-negative wives disclosure their serodiscordant relationship, especially to nurses and other health care providers, may become a challenge for HIV prevention programs within a household. As a care provider who counsels Muslim wives on HIV testing, a nurse needs to understand HIV-related stigma among Muslim wives and their coping strategies to develop HIV prevention programs or interventions.
Methods
Study Design
The study was a part of the doctoral dissertation entitled ‘sexual negotiation for HIV prevention among Muslim married women within serodiscordant relationships in the Indonesian socio-cultural context’ using a grounded theory approach (Agnes et al., 2018).
Participants
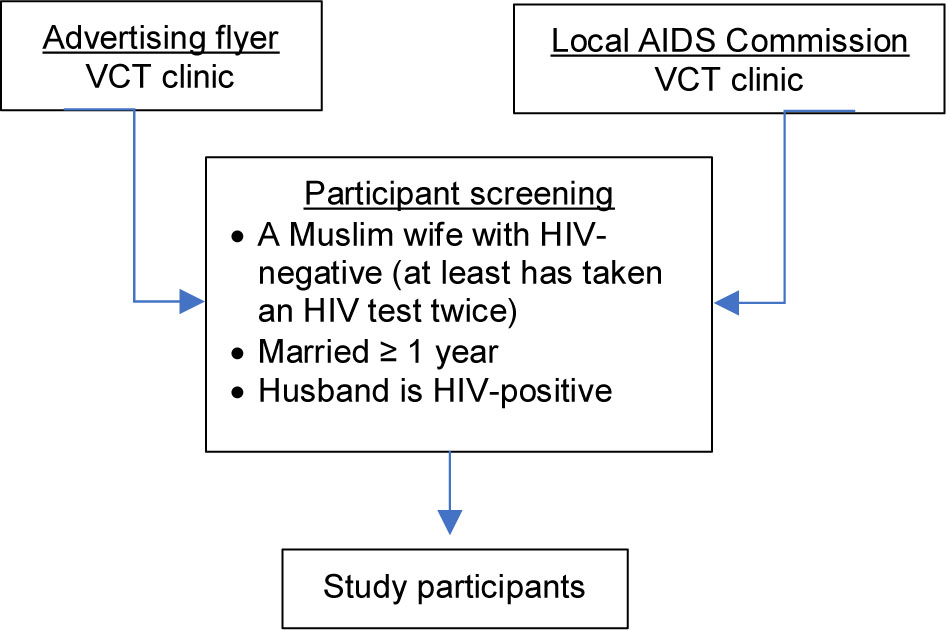
The study initially used purposive and snowball sampling approaches to recruit participants. Seven of the total HIV-negative wives with experiences of HIV-related stigma were selected from the more extensive study. The eligibility for participation was chosen by following inclusion criteria: being a wife with an HIV-positive husband (based on the Non-Governmental Organization (NGO) / Voluntary and Counseling Testing (VCT) clinic reports), being married for at least one year, and was taken an HIV test at least twice. There were two pathways to obtain access to the eligible participants. The first recruitment pathway was through VCT clinics at public hospitals in two towns (Blitar District and Kediri Municipality). The second recruitment pathway was through Non-Government Organizations (NGOs) working on HIV/AIDS (all members of the NGO were HIV-positive) (Figure 1).
Data Collection
Data were collected over 15 months between April 2016 and July 2017 through in-depth interviews, observation, and field notes. Each participant was interviewed by the researchers at least twice, mainly at the participants’ homes. Each interview was about 60 minutes and recorded using a digital recorder. A guideline for the interview in open-ended questions in Bahasa Indonesia was used. The sample questions included “what did you perceive about your husband’s illness”? “what was your family’s reaction when they knew your husband’s HIV status?” Recorded interviews were transcribed verbatim in Bahasa Indonesia for analysis. In addition, participants’ behavior and nonverbal communication during the interviews were recorded in the field notes. Data collection and data analysis proceeded simultaneously until no more new information.
Data Analysis
Data were analyzed according to the guidelines of constructivist grounded theory with the process of initial coding, focusing coding, theoretical coding, memo writing, theoretical sampling, saturation, and ordering memos (Charmaz, 2006). Line-by-line coding was applied for all the manuscripts in the initial coding. All of the codes from the transcripts were written down in different electronic worksheets to develop preliminary categories. In the process of focused coding, the researchers reviewed the codes used by the participants from the initial coding. During this process, memo writing was performed, and all codes from the initial coding were reviewed and grouped similar codes into preliminary subcategories. One core category was determined in the theoretical coding process. The saturation was reached when the researcher extended to sample and code data until no new categories can be identified and up to when new cases of variation for the existing categories have stopped arising (Kyngäs et al., 2020).
Trustworthiness/Rigor
For a study to be trustworthy, Patton (2015) identifies five essential elements; credibility, authenticity, dependability, conformability, and transferability. To increase conformability, the researchers can use processes such as data audits (Patton, 2015). In this study, the various forms of data were collected from personal interviews and observations. The participants’ quotes were used to confirm the categories, in which used in theory. Therefore, the categories emerged from the participants’ experiences and were not solely based on the researcher’s interpretation. To ensure dependability, detailed memos before the beginning, during the planning stages, during the discussion sessions, after each session were provided. Peer review with faculty advisors to confirm emerging themes also helped to support the dependability of the results. To ensure credibility and conformability, a member checks whether the codes and categories were valid to the participants’ experiences. The participants performed a second review of the codes, grouped codes, and concepts as a member check. The intent of transferability is to transfer findings from one context to another. By offering rich narratives and thick descriptions of context and participants and clearly stating the purpose of the study, transferability to other individuals and/or situations becomes a viable result of the qualitative research process (Patton, 2015). In this study, a prolonged engagement with the participants and their atmosphere helped the researcher gain their trust and more personal data.
Ethical Consideration
The study was approved by an Institutional Review Board committee of University No MOE 0521.1.05/2148. All participants were informed of the study’s objective, and they signed a free and informed consent form. They also were informed about the purpose and the nature of the study, participant’s rights, confidentiality, and potential risks of the study. All information was delivered through oral and information sheets. Oral information was provided in two languages, both Javanese (the local language in the study setting) and “Bahasa Indonesia” (national language). The crucial issue in joining the study was that some husbands wanted to accompany their wives whenever the researchers did the interview. In this case, the researchers placed the husband in a different area but still at the exact location of the interview and asked the HIV/AIDS activists to accompany the husband during the interview.
Results
Characteristics of the Participants
The key participants of the study were seven married Muslim women with HIV-positive husbands. The participants’ age ranged between 26 and 48 years old. Javanese was the most common ethnicity of the participants (100%). The majority of the participants (57%) were housewives, in nuclear families (87%) and extended families (13%). All of the participants reported knowing their husbands’ HIV-positive status during their marriage.
Thematic Findings
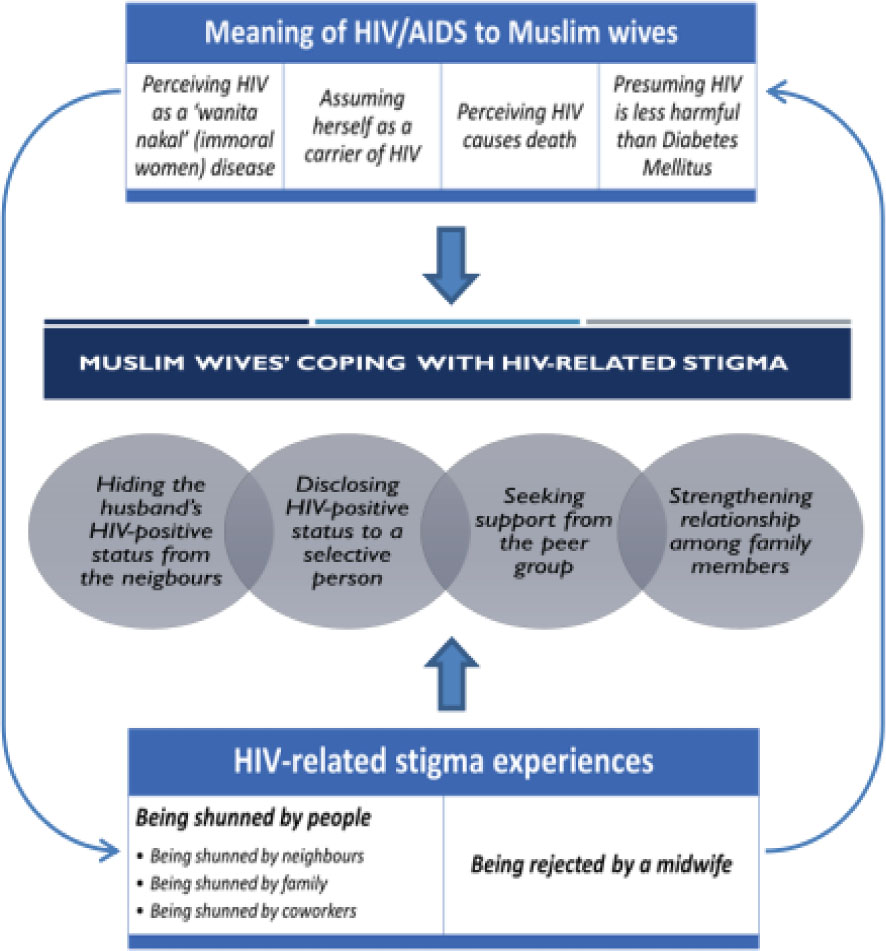
Three themes emerged from the data based on the aim of the study: 1) the meaning of HIV/AIDS to Muslim wives, 2) HIV-related stigma experiences, and 3) Muslim wives’ coping with HIV-related stigma (Figure 2).
Theme 1: Meaning of HIV/AIDS to Muslim wives
Muslim wives’ perceptions of HIV/AIDS had been shaped by the negative perception of HIV/AIDS in society. All of the participants associated HIV/AIDS with immoral behaviors, such as sex workers. Some participants perceived they might be responsible for their husbands’ illness because of their history as international migrant workers. Another participant perceived that her status as a divorcee might lead her recent husband to get HIV. They also believed that people with HIV/AIDS would be dying soon after the diagnosis. However, some participants were less worried about their husband’s illness because they compared it to another disease.
Perceiving HIV as a ‘wanita nakal’ (immoral women) disease
Participants’ perceptions about HIV might represent how society stigmatized HIV/AIDS as a wanita nakal (immoral women) disease. In the participants’ community, wanita nakal (immoral women) was identified as female sex workers (FSWs). Therefore, they perceived that only wanita nakal could get the disease. As a result, they could not believe it when they received their husband’s diagnosis. The following participant’s quotation was an example of the participant’s perception of HIV/AIDS:
When my husband told me he got HIV, I did not believe it. At that time, I believed only wanita nakal could get the disease. That is what people said about HIV (Mrs. L, age 36)
Assuming herself as a carrier of HIV
Two of the participants were concerned they might be blamed for their husbands’ illness. They perceived having some responsibilities because of their backgrounds. Being a divorcee and a migrant worker made them feel that they had put their husbands at risk of HIV transmission. The participants talked about their worries:
I thought he got HIV from me, yet I never had sex with other men before he married. Still, if people knew he got HIV, they would blame me because I used to work as a migrant worker in Taiwan. People said that if someone used to work as a migrant worker, she might have HIV (Mrs. W, age 43)
For me, I could tell that I might also share the risk fifty-fifty since I was a divorcee when I married him so that I could transmit the disease as well (Mrs. R, age 26)
Perceiving HIV causes death
Most of the participants believed that HIV was like a death sentence. People living with HIV/AIDS (PLWHA) would die soon. For example, some of the participants thought they would lose their husbands soon because, at the time they received the news about their husband’s HIV-positive status, their husbands were very sick. For example, Mrs. I, a 42-year-old housewife, explained her worries as follows:
I felt shocked when I heard about my husband’s HIV status for the first time. At that time, I thought my husband would die soon. I cannot imagine how I would be bringing up my son alone if he died (Mrs. I, age 42)
Presuming HIV is less harmful than Diabetes Mellitus
Two participants perceived the HIV was better than Diabetic Mellitus (DM). The meaning was relatively favorable for self, influenced by health care providers who advised their husband’s illness was HIV-positive. They also got information that DM was more dangerous than HIV/AIDS. They explained their husbands’ HIV-positive status to their families by using this comparison. Some of the participants shared their understanding of HIV/AIDS:
For me, HIV is not easily contagious. Diabetes is a more dangerous disease than HIV (Mrs. T, age 45)
Our families knew about my husband’s HIV status and accepted. There was no negative response. The doctor said my husband’s illness was less severe than diabetes (Mrs. S, age 48)
Theme 2: HIV-related stigma experiences
The participants had many bad experiences related to their husband’s HIV-positive status. Being shunned and away from others was a shared experience. People rejected and avoided HIV-positive persons and their families, even if the family members were HIV-negative. Another participant was rejected by a health care provider when she wanted to do antenatal care and get a vaccine for her children. The HIV-related experiences of the participants can be categorized into:
Being shunned by people
Most of the participants experienced being avoided by their extended family, neighbors, and coworkers when the news about their husband’s HIV status spread thoroughly. For example, one of the participant’s families who lived next to the participant was relocated to another place to avoid her husband.
Being shunned by neighbors
Our neighbors did not want to talk to us. When I tried to talk to them, they would answer from a distance as necessary. It was better than before. At first, my neighbors did not want to speak to us when my husband was just released from the hospital. They did not want to visit us. All of my neighbors already knew that my husband is HIV-positive (Mrs. Sun, age 41)
Being shunned by family
Even two of my husband’s siblings and their family moved out from their home since our houses are close. They moved out to another place since my husband was released from the hospital. They stayed with one family for a while then went to another family. They were very worried my husband would transmit the disease to them. They perceived that the disease would be transmitted through the water. Very funny (Mrs. Y, age 35)
The worst thing was that his siblings did not want to visit him, but they also prevented people from visiting us. Those people said that they would get the disease by talking to us. My relatives had the same opinion (Mrs. Sin, age 41)
Being shunned by coworkers
Even though my husband works at Puskesmas (Primary Health Care service), his coworkers are avoiding him since he knows he is HIV-positive. I do not know why they act like that. They work at a health care service. They should know better about HIV/AIDS than we (ordinary people) do. However, what can I do? It is difficult to change people’s minds (Mrs. Sun, age 41).
Being rejected by a midwife
One of the participants received discrimination from the midwives during her pregnancy because of her husband’s HIV-positive status. As a result, she was rejected when she came to a midwife for a pregnancy check-up.
We found out about my husband’s HIV status when I was pregnant with my second child. I did not know where the midwives got the news. She rejected me when I came to the clinic for a pregnancy check-up. She asked me to go to the hospital instead. I felt hurt. The hospital is very far… Very, very far. It would take more than one hour to go there, and the road is not in good condition. I told her that my HIV status is negative. However, she still insisted I should go to the hospital for a pregnancy check-up. She is a health care provider. She should know better. Why she treats me like that? It was getting worst when I was pregnant with my third child. After we knew about his HIV and all the bad experience we had during my second pregnancy, we decided not to have another child. However, Allah has another plan for us. I was pregnant again. All the midwives in our area refused to do a pregnancy check-up on me. (Mrs. Lk, age 36)
One of the midwives even scolded me about my pregnancy. She claimed that I should not be pregnant again because of my husband’s HIV status. I felt hurt, really hurt. The midwife even did not want to immunize my children (Mrs. Lk, age 36)
Furthermore, Mrs. Lk was very upset with the midwives because of the irrational accusation about the cause of her husband’s illness.
So, when I was pregnant with my second child, a midwife came to our house because of my pregnancy and my husband’s HIV status. At that time, she asked us many things related to HIV/AIDS as if she did not know about it. Then she railed on my husband’s HIV status. It seems she accused my husband has had sex with a sex worker from whom my husband got HIV. I was very mad at her. She did not know my husband, yet she accused him. I was upset, but I said nothing at that time. (Mrs. Lk, age 36)
Theme 3: Coping strategies of HIV-related stigma
In this study, all of the participants tried to be strong for their families. As a wife, all of the participants were being main caregivers for their husbands. Some participants chose to talk to their families, while other participants kept the news to themselves. Some participants came to their families (parents, siblings, brothers-in-law, sisters-in-law) to find the strength to face their new life with their HIV-positive husbands.
Hiding the husband’s HIV-positive status from the neighbors
Hiding the husbands’ HIV-positive status was a main concern for the participants. In their situation, they could not leave their husbands without revealing their husbands’ HIV-positive status to their family and friends. They could not use their husbands’ illness as a reason to leave their husbands. Instead, they chose to commit to their husbands and marriages. Three participants decided to keep news about their husbands’ illness for themselves. They did not want their extended families and neighbors to hear about their husbands’ illness. The participants believed that if people knew about their husbands’ HIV status, their families would avoid them. They felt shame because HIV was an immoral disease. One participant, a 36-year-old housewife, explained her situation as follows:
I did not tell anyone about my husband’s illness, even my own family. I kept it for myself; I did not tell my neighbors. No one knew about my husband’s illness. It would be a shame if my neighbors knew about it. They would avoid my family as well (Mrs. LI, age 36)
Another participant, a 46-year-old housewife, mentioned that she kept her husband’s illness from her family and neighbors. She told them that her husband got chronic gastritis whenever her neighbors asked about her husband’s illness.
I told my daughter and neighbors that my husband gets chronic gastritis. I did not want my daughter to know about her father’s illness. It will make her upset. If my neighbors know about my husband’s illness, I am worried that they avoid my family. Whenever they come to visit my husband, they always asked about his illness. I just told them that he has chronic gastritis. They seemed to believe it (Mrs. MA, age 46)
Disclosing HIV-positive status to a selective person
Disclosing to a selective person referred to an act of telling a certain person whom they believed could be trusted to keep their secret and also to get the support they needed. Four participants shared the news of their husbands’ illness with their families. They revealed their husbands’ HIV-positive status to their brothers or sisters-in-law, their children, parents, and extended families. The following participants’ quotations provide examples:
Until now, we only tell our firstborn and my husband’s twin. When I told my firstborn about his father’s illness, he was also shocked. Fortunately, since he is a grown-up, we ask him to keep the news for himself (Mrs. Sun, age 41)
I told my husband I could not bear the news alone, and I asked him whom we should tell about his illness. There are two choices, his mother and his older sister. Then he decided to tell his older sister. So, when his sister came to visit, we told her that he got HIV (Mrs. Sy, age 41)
I told my sister-in-law about my husband’s illness. She is supporting us financially and took care of all the hospital bills. She was very grateful to me because I took care of his brother and did not leave him after he got the illness (Mrs. At, age 38)
Furthermore, one of the health care providers stated that disclosing their husbands’ HIV-positive status was an important factor in the household. The HIV disclosure was the first step the husband took to protect the wife from HIV.
The first thing is that the husband has to open up to his wife. There were many cases in which the husbands came to the clinic and took the test. After they knew the result, they kept it to themselves. The husbands did not want to inform their wives. In the end, their wives knew their husband’s HIV status after the husband had passed away. Some of the wives came to the hospital because they had similar symptoms before the husband died. One wife took an HIV test, and the result was positive (Counselor, age 30)
However, the disclosure of the husband’s HIV-positive status has its consequences. Two of the participants were suggested by their families to leave their husbands when informed of their husbands’ illness.
When my mother knew about my husband’s illness, she asked me to divorce him (Mrs. R, age 26)
In the end, I talked to my siblings. Some of my siblings suggested I divorce my husband. Other siblings said I had to consider my financial situation if I wanted to divorce him since I have no job, and there is a huge need for my children’s education. I was very confused (Mrs. Nur, age 45)
Moreover, other participants were avoided by their extended family after they knew about their husbands’ HIV-positive status. They explained that their extended family did not come to visit their husbands anymore. Some of the extended family only called them by phone to update them on the news about their husbands. In Javanese culture, it is very common for family members to take care of each other whenever their family is in a difficult situation. Member of the family does not wait to be asked for help. They will come and by themselves and do everything that needs to be done based on their capability. One participant, a 35-year-old housewife, explained the attitude of her extended family after they knew about her husband’s HIV-positive status.
When my husband was hospitalized, I went along with him; and left my children at home by themselves. There was no one to step in and take care of my children. In the past, before my husband’s family knew about his HIV status, they always took care of my children whenever my husband was admitted to hospital. I felt miserable (Mrs. Y, age 35)
Seeking support from the peer group
The participants communicated with the peer group facilitators for PLWHA since they often come together with their husbands to attend a monthly meeting. They found out the peer group was beneficial. The participants felt free to discuss their husbands’ illness with the peer group’s facilitator because they were in the same situation. The peer group support made them able to deal with their husband’s illness easier. Having someone on whom they could depend relieved their worries. One participant, a 41-year-old kindergarten teacher, expressed her feelings as follows:
Alhamdulillah (thanks to Allah), Joko (a facilitator from a peer group), is always there whenever I want to talk about my husband’s illness. It is impossible to talk to my family or my neighbor if something happens to my husband. I always call Joko. I do not know what I would do with my husband if there were no Joko. Alhamdulillah, he can always be reached. So, whenever I want to ask something, I call him. I only can consult with my husband’s doctor when we visit the clinic. Joko is very helpful (Mrs. Sun, age 41)
Strengthening relationship among family members
The participants decided to share the news with other family members because of the need for support for being a caregiver and helping if something happened to their husbands and they could not face it alone. They obtained varied responses from their families. The responses might indicate how close the relationship between the participants and their families is. Five participants gained support from their husbands’ families.
I told my husband’s brothers about his illness, and they helped me take care of him every day (Mrs. T, age 45)
I told my eldest son about his father’s illness to help me if something happens to my husband. By knowing his father’s illness, I want my son will be more careful. My son always drives his father to the hospital for a monthly check-up and to take medicine. He has the right to know about his father’s illness (Mrs. Sun, age 41)
I told my kids that their father got HIV. I need their help to take care of him. I do not want my kids to hear about their father’s illness from others. Even though my kids are angry about the current situation, they are always eager to help me when I need it (Mrs. L, age 36)
Discussion
This study sought to understand the experiences of HIV-related stigma faced by HIV-negative Muslim wives in serodiscordant relationships and their coping strategies. All of the participants perceived that HIV is a ‘wanita nakal’ (immoral women) disease. Their perception was congruent with a previous study that found two HIV-positive sex workers in a brothel in Surabaya, East Java Province, Indonesia. Since then, the Indonesian community has begun to perceive HIV as a disease of female sex workers, known as ‘women without morals’ (wanita tuna susila) (Imelda, 2011). This negative perception is so bad that when women were found to have HIV, they were accused of immoral sexual behavior and rebellious toward religious teachings. However, if the husband got HIV, the wife was accused because of her incapability to fulfill her husband’s sexual needs, which lead the husband to seek sex with another woman (Sciortino et al., 1996). Some of the participants even assumed they were the ones who had transmitted HIV to their husbands because of their background before marriage. They perceived that being a widow and ex-female migrant worker put them at risk of HIV carriers. All of the participants had married Javanese men and lived in the Javanese community. Their marital relationships within the Javanese family are influenced by Javanese culture in which women should support their husbands; they remained to idealize a ngabekti-ngayomi (devotion-protection) relationship with the husband. This philosophy affected how the participants reacted and took action in overcoming the problems caused by the stigma.
The findings showed that HIV-negative Muslim wives experienced several forms of HIV-related stigma after people knew about their husband’s HIV-status. They were avoided by their family, neighbors, and coworkers. As shown in other studies, stigmatization was often based on fear of contracting the disease (Siegel et al., 2018; Mahamboro et al., 2020). Being rejected by health care providers was also another experience faced by the participants. As reported in previous studies, the rejection is most likely because of a lack of knowledge about the transmission and irrational judgment of the health care providers (Chambers et al., 2015; Qonitatillah et al., 2020). Since HIV/AIDS and reproductive health are mandatory in every health education program in Indonesia, the lack of knowledge and irrational judgment related to HIV/AIDS are noteworthy.
Furthermore, the study also found that some of the participants were advised to leave their husbands to avoid transmission. Another reason was because of people’s perception of HIV/AIDS. This finding is similar to several previous studies when family and friends suggested the HIV-negative party leave their partner (Bourne et al., 2017; Siegel et al., 2018). In this study, Islamic and Javanese values might play a role in participants’ decision to not leaving their husbands. In Islam, marriage is a religious task and is consequently a moral safeguard because families are established through marriage (Dogarawa, 2009). Therefore, while a divorce is allowed in Islam, it is most hated by Allah (Abu Dawud and Ibn Majah as cited in Jaafar-Mohammad & Lehmann, 2011). Furthermore, Indonesian society has a stigma attached to being a widow (janda mati) or divorcee (janda cerai). Society has stigmatized a janda (a widow or divorcee) as an immoral woman. It is hard for such a person to hold herself as a respectable woman (Parker et al., 2016).
Regardless of the bad experiences of HIV-related stigma, HIV-negative Muslim wives were able to produce some strategies. They overcome the stigma by disclosing their husband’s HIV status to a certain person, which is beneficial. All of the participants shared their husband’s HIV status with someone (family members, close friends) to prepare themselves if the worst happens and get the help they needed. This finding is supported by a previous study that people will gain a support system when they disclose their situation to family, friends, and coworkers (Kasapoglu et al., 2011).
Furthermore, some of the participants also connected to the peer group of PLWHA to gain more knowledge related to serodiscordant relationships. They felt comfortable discussing their situation among people with the same situation as them. As described in another study, when HIV-negative partners in serodiscordant relationships fear rejections from their family or friends, they may choose to seek support within their HIV-positive partners’ peer group or HIV community organizations (Talley & Bettencourt, 2010).
The researchers found there were some limitations in this study. First, this study focused on HIV-negative Muslim women with HIV-positive husbands in the Javanese community. Another limitation was that the women participants were asked to recall events that could have occurred several years ago. Therefore, it is necessary to acknowledge serodiscordant couples in other ethnicities and explore their experiences toward HIV-related stigma.
Conclusion
The study identified several ways to address HIV-related stigma among HIV-negative Muslim wives. Since the stigma is experienced by persons differently, it should be addressed from different angles and aspects. The findings are important as supporting serodiscordant couples can be beneficial in the fight against HIV/AIDS and HIV-related stigma. Therefore, a study on the experiences of HIV-related stigma among HIV-negative Muslim wives in a serodiscordant relationship and their strategies to manage HIV-related stigma was very much needed. In addition, this study contributed to nursing science by providing nurses with an understanding of the experience of disclosure of HIV-negative wives in a serodiscordant relationship in a Muslim context. Nurses in the community played an essential role in decreasing the number of HIV infections among married women.