










Background
Occupational stress is a major health and economic issue, with widespread impacts on individual workers’ health and wellbeing, families, workplaces, and financial/economic stability. Well-described impacts for the individual include increased absenteeism, poorer job performance, work dissatisfaction, and stress symptoms (Peter et al., 2020). For health care settings, decreased productivity and absenteeism can have widespread and costly impacts on the workforce and those receiving care. Nurses experience higher rates of job stress compared to other professionals, with accompanying increased turnover, absenteeism (Kaddourah et al., 2018; Peter et al., 2020), and increased prevalence of chronic health problems (Deng et al., 2020). Not only does nurse-related job stress affect individual nurses’ health and increase costs from replacement staff salaries, but it can also influence patient care and patient satisfaction. This, in turn, can influence recovery and increase the risk for medication or treatment errors (Martin, 2015).
In Bangladesh, approximately 4.1% of the general population had depression, and depression accounted for 7.1% of total years of life lived with disability in Bangladesh (World Health Organization, 2017). Recently, one study found that 80% of Bangladeshi nurses experienced stress at work, and 40% had depressive symptoms (Salma & Hasan, 2020). Studies completed in other countries found that the prevalence of depressive symptoms is higher in Registered Nurses (RNs) than in the general population (Hall et al., 2018). Significant levels of depressive symptoms in RNs have been reported, 35.8% in China (Cheung & Yip, 2015) and 32.4% in Australia (Maharaj et al., 2019). Using diagnostic criteria, the one-year prevalence rate of Major Depressive Disorder (MDD) among Canadian nurses was 9.3% (Enns et al., 2015).
Specific work environment-related factors, including work overload and conflicts with physicians or other nurses, have been identified as contributors to depressive symptoms (Hall et al., 2018). In addition, several individual characteristics of nurses also were found to be associated with depressive symptoms, including age, marital status, professional education, and specialization practice settings (Khodadadi et al., 2016). The existing evidence indicated that nurses use problem-focused and emotion-focused coping strategies to deal with stressful situations (Li et al., 2017). Chen et al. (2020) found there was a significant association between coping and depression.
As the largest component of the health care workforce, it is critically important for health care settings and administrators to proactively consider strategies to attenuate occupational stress within the traditions, culture, and context of a specific health care system and the practice settings within that system. Potential strategies must be based on information obtained within a specific country, culture, and health care environment. Our overall aim was to fill that information gap specifically as it relates to Registered Nurses (RNs) in Bangladesh by initiating the first of a series of studies, beginning with a survey of RNs examining sources of work-related stress, how RNs coped with such stressors, and potential relationships among sources of work-related stress and depressive symptoms.
The present study was guided by the Transactional Theory of Stress and Coping (Lazarus & Folkman, 1984), which explains stress through the relationship patterns among three major concepts. These concepts include a cognitive appraisal, coping, and adaptational outcome. Cognitive appraisal is a process of evaluation to determine why and to what range a specific transaction or series of transactions between the person and the environment is stressful. Coping is a dynamic process that changes as the appraisal of the person-environment relationship changes over time based on the situation. This process can be a two-way process that alters the problem (problem-focused coping) and regulates the emotion behavior (emotion-focused coping). The long-term inability to cope with the situations may have an impact on adaptational outcomes, including psychological wellbeing, social functioning, somatic health, and illness of a person. In this study, workplace stress was used for cognitive appraisal while coping as a process of coping. The depressive symptoms were used as the adaptational outcome.
Our objectives were to examine (1) frequency of depressive symptoms as a common outcome of occupational stress; (2) the relationship among depressive symptoms, the various individual and system sources of work-related stress and coping strategies used by participants, and (3) the potential mediating roles of coping strategies in the relationship between workplace stress and depressive symptoms.
Methods
Study Design
This study used a correlational research design with a cross-sectional approach.
Participants
The population was RNs who had been working at governmental MCHs in Bangladesh. The sampling selection using proportional stratified random sampling with inclusion criteria: 1) respondents employed in the selected hospital for at least one year, and must have worked in the current unit for at least three or more months; 2) respondent is providing direct care for hospitalized patients. Exclusion criteria were nurses worked as a manager/supervisor or in the operating room or outpatient department and nurses currently on a long-term absence.
The sample size was determined by the power analysis method using G*Power 3.1 (Faul et al., 2007) based on a previous study (Tsaras et al., 2018). Three hundred and sixty respondents were needed for a two-tailed analysis using logistic regression with a .05 alpha level, 80 power, and 1.904 odds ratio. The questionnaires were distributed to 416 nurses, of which 360 sets were returned, translating to a response rate of 86.54%. A total of 8 questionnaires were incomplete and thus excluded from the analyses, leaving 352 sets eligible for data analyses.
Instruments
Demographic questionnaire. Respondents completed a demographic questionnaire that included age, religion, marital status, the highest level of professional education, work experience as a nurse, working experience in the current hospital, sufficiency of personal monthly income, number of children, and living arrangements.
Nursing Stress Scale (NSS) (Gray-Toft & Anderson, 1981), a 34-item questionnaire was used to measure seven different sources of workplace stress include: 1) Death and dying 2) Conflict with physician 3) Inadequate preparation 4) Lacks of support 5) Conflict with others nurses 6) Work overload and 7) Uncertainty about patient care. It is a 4-point Likert scale, responses range from 0 = [never] to 3 = [very frequently]. The sum of higher scores indicated that the nurses experienced higher levels of workplace stress. The value of Cronbach’s alpha was .84.
Ways of Coping Questionnaire (WCQ) (Folkman & Lazarus, 1988a, 1988b), a 50-item questionnaire was used to assess the individual’s use of eight different strategies of coping: 1) Confrontive coping; 2) Distancing; 3) Self-controlling; 4) Seeking social support; 5) Accepting responsibility; 6) Escape-avoidance; 7) Planful problem-solving; and 8) Positive reappraisal. In addition, the WCQ groups the items into two more general styles of coping (problem-focused coping and emotion-focused coping) (Folkman & Lazarus, 1985). The WCQ is a 4-point Likert scale, with responses ranging from 0 = [does not apply or not used] to 3 = [used a great deal]. The sum of higher scores indicated that the person frequently used the behaviors and cognitive strategies described by that scale during coping with a stressful event. The value of Cronbach’s alpha was .92.
Center for Epidemiologic Studies-Depression (CES-D) (Radloff, 1977), a 20-item questionnaire, was used to measure depressive symptoms. The CES-D is a 4-point Likert scale, with responses ranging from 0 = [rarely or none of the time] to 3 = [most or all of the time]. The sum of higher scores indicated more symptoms of depression. The CES-D scale categorized depressive symptoms based on: not depressed (0-16); depressed (> 16). The value of Cronbach’s alpha was .80.
All instruments used in this study are original English versions, which received permission from the authors.
Data Collection
Data collection was carried out by the first author from March to June 2017 at four governmental MCHs in Bangladesh.
Data Analysis
Data were analyzed using SPSS version 18 software. Descriptive statistics summarized demographic and relevant study variables. A logistic regression analysis was used to explore the association among depressive symptoms, workplace stressors, and personal characteristics with a significance level of p <.05. Baron and Kenny’s method was used to test the mediating effect of coping on the relationship between workplace stress and depressive symptoms (Baron & Kenny, 1986).
Ethical Consideration
The study was approved by the Institutional Review Broad of Faculty of Nursing, Mahidol University, Thailand (COA. No. IRB-NS 2017/398.0602), and ethical clearance was obtained from the authorities of the selected Bangladeshi MCHs. Informed consent was signed by each participant prior to data collection.
Results
Table 1 summarizes the demographic information of the participants. There were no young early career participants (average age was 41, range: 29-59). Most were female and married. Two-thirds of the nurses (68.5%) were Muslim. Three-quarters of the RNs were diploma-prepared and had worked an average of 18 years as an RN. The four types of patient units were equally represented, and the average work experience in the current hospital was 10.9 years. Most of the participants lived with their spouses and children and reported that their personal income was insufficient.
| Personal characteristics | % (N) | Mean (SD) | Range |
|---|---|---|---|
| Age (in years) | |||
| 29-39 | 44.6 (157) | 40.1 (6.6) | 29-59 |
| 40-49 | 45.2 (159) | ||
| 50-59 | 10.2 (36) | ||
| Religion | |||
| Muslim | 68.5 (241) | ||
| Hindu | 30.1 (106) | ||
| Christian | 1.4 (5) | ||
| Marital status | |||
| Married | 90.3 (318) | ||
| Single | 6.8 (24) | ||
| Others | 2.9 (10) | ||
| Professional education | |||
| Diploma in Nursing | 74.7 (263) | ||
| B.Sc. in Nursing/PHN | 13.4 (47) | ||
| MSN/MPH | 11.9 (42) | ||
| Experience as a nurse (in years) | |||
| < 10 | 13.4 (47) | 18.1 (7.1) | 2-38 |
| 10-19 | 55.1 (194) | ||
| 20-29 | 28.4 (100) | ||
| >30 | 3.1 (11) | ||
| Years in current hospital | |||
| 1-9 | 51.4 (181) | 10.9 (8.4) | 1-32 |
| 10-19 | 32.1 (113) | ||
| > 20 | 16.5 (58) | ||
| Personal monthly income | |||
| Sufficient | 40.6 (143) | 40.6 | |
| Insufficient | 59.4 (209) | 59.4 | |
| Number of children | |||
| 0 | 10.8 (38) | ||
| 1-2 | 82.4 (290) | ||
| 3 | 6.8 (24) | ||
| Number of family members living with participant | |||
| Only respondent | 4.3 (15) | 4.3 | |
| 1-4 | 68.5 (241) | 68.5 | |
| 5-6 | 24.1 (85) | 24.1 | |
| 7-8 | 3.1 (11) | 3.1 |
Table 2 summarizes the data obtained from the three standardized self-reports, including the means and standard deviations (SD) of the total scores, as well as the means and SD for the subscale scores for the NSS and WCQ and the calculated reliability coefficients. Although the overall average score for the entire sample on the CES-D was 15.73 (SD = 6.09), 51.4% of the RNs had scores of ≥16, equaling or exceeding the established cut-off score significantly correlated with MDD. The mean score in the subgroup of participants (N = 181) who had scores ≥16 was 20.35 (SD = 4.73).
| Scores | Mean | SD | Cronbach α |
|---|---|---|---|
| CES-D total score | 15.73 | 6.09 | .80 |
| NSS total score | 50.67 | 11.36 | .84 |
| WCQ total score | 52.68 | 17.30 | .92 |
| NSS2 subscales (number of items) | |||
| Workload (6) | 10.88 | 2.79 | .49 |
| Death and dying (7) | 11.62 | 3.53 | .67 |
| Uncertainty regarding Treatment (5) | 8.10 | 2.79 | .62 |
| Inadequate preparation (3) | 4.78 | 1.45 | .56 |
| Conflict with physician (5) | 7.16 | 2.76 | .66 |
| Lack of support (3) | 3.13 | 1.48 | .32 |
| Conflict with other nurses (5) | 4.91 | 2.27 | .44 |
| WCQ4 subscales (number of items) | |||
| Seeking social support (6) | 8.79 | 2.07 | .47 |
| Planful problem solving (6) | 8.39 | 2.44 | .53 |
| Positive reappraisal (7) | 9.52 | 3.02 | .65 |
| Accepting responsibility (4) | 4.38 | 1.87 | .46 |
| Escape-avoidance (8) | 5.00 | 3.66 | .75 |
| Confrontive coping (6) | 5.32 | 3.07 | .68 |
| Self-controlling (7) | 6.23 | 3.55 | .77 |
| Distancing (6) | 4.91 | 2.67 | .68 |
| Escape-avoidance (8) | 5.00 | 3.66 | .75 |
| Coping scores grouped by: | |||
| Problem-focused coping (25) | 29.4 | 8.5 | .85 |
| Emotion-focused coping (25) | 20.53 | 10.15 | .90 |
The average score for the NSS was 50.67 (SD = 11.36). The most frequent sources of workplace stress (in rank order from highest to lowest) were Work Overload, followed by Death and Dying and Uncertainty regarding Treatment Care (Table 2). Conflict with Other Nurses and Lack of Support were perceived as the least stressful aspects of their workplace. The total mean score of the WCQ was 52.68 (SD = 17.30). The three coping strategies perceived to be most commonly used (by rank order from the most frequently used) included Seeking Social Support, Planful problem solving, and Positive reappraisal. Confrontive coping, Self-controlling, and Escape avoidance were deemed the least commonly used. When the WCQ items were dichotomized into the problem- or emotions-focused coping strategies, the mean of problem-focused coping strategies was 32.08 (SD = 8.44), and the mean of emotion-focused coping strategies was 20.56 (SD = 10.21). Table 2 also summarizes the calculated reliability coefficients for the NSS and the WCQ and their subscales.
Table 3 provides information regarding relationships among age, marital status, professional education, working unit, and workplace stress and depressive symptoms. A significant positive association was found between NSS scores and depressive symptoms [odds ratio (OR) 1.05, 95% confidence interval (CI) 1.03, 1.08, p < .01]. However, personal characteristics including age, marital status, professional education, and working unit were not associated with depressive symptoms.
| Variables | B | S.E. | p-value | OR | 95% CI | |
|---|---|---|---|---|---|---|
| LL | UL | |||||
| Age | .01 | .02 | .69 | 1.01 | .97 | 1.04 |
| Marital status (ref: divorce, widowed, and separate) | ||||||
| Single | -.09 | .82 | .92 | .92 | .19 | 4.56 |
| Married | -.20 | .71 | .78 | .82 | .21 | 3.28 |
| Professional education (ref: M.Sc. Nursing/PHN) | ||||||
| Diploma in Nursing | -.11 | .36 | .77 | .90 | .44 | 1.83 |
| B.Sc. in nursing / PHN | -.24 | .46 | .60 | .79 | .32 | 1.93 |
| Working Unit (ref: Gynae/Obstetrics) | ||||||
| Medical unit | -.31 | .34 | .37 | .73 | .38 | 1.43 |
| Surgical unit | -.38 | .33 | .24 | .68 | .36 | 1.29 |
| Critical care unit | -.06 | .32 | .86 | .95 | .50 | 1.78 |
| NSS total score | .05 | .01 | .01* | 1.05 | 1.03 | 1.08 |
| Reference category | Non-depression | |||||
| Pseudo R2 | .073 | |||||
Legend: * = significant (p ≤. 05)
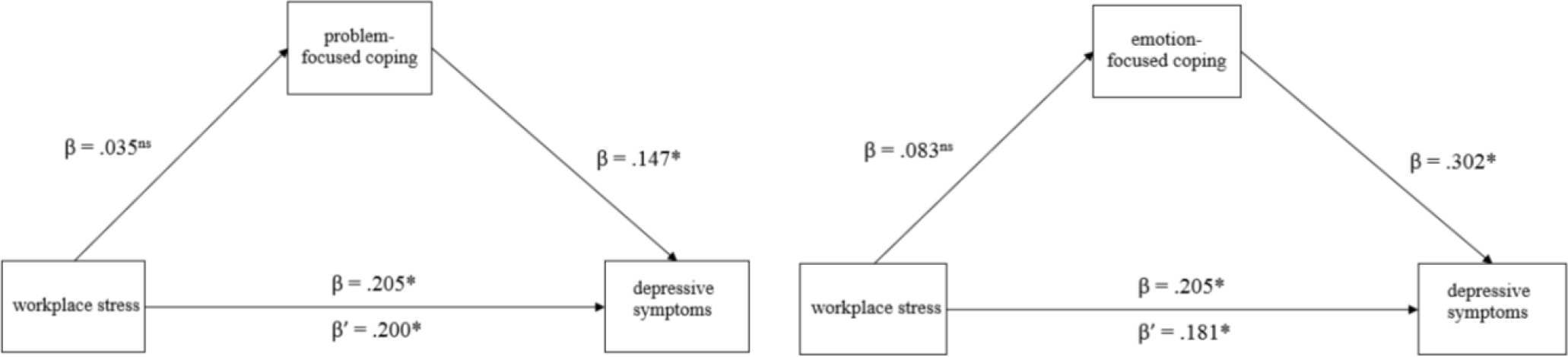
Figure 1 show significant relationship between workplace stress and depressive symptoms (β = .205, p < .05) before controlling the mediating variable. When the mediating variable was controlled, the results showed that the relationship between workplace stress and depressive symptoms was still significant (β/ = .200 and .181, p < .05). It means that there were no mediating effects of either problem- or emotion-focused coping scores on the relationship between workplace stress and depressive symptoms.
Discussion
The major finding that more than half of the nurses (51.4%) scored greater than 16 on the CES-D (mean 20.35, SD = 4.73) is alarming. Similar to the study with Chinese RNs (Li et al., 2017), the fact that half of the RNs that participated in the study (representing 12% of the overall pool of RNs) are likely experiencing MDD should be a call to action on the part of hospital administrators and unit managers. To add support that the work environment contributed to depressive symptoms is the positive relationship between the total scores on the NSS and CES-D.
Other sources of stress (e.g., home environment, financial insecurity, personal relationships, and chronic health problems) may also make a significant contribution to the risk of developing depressive symptoms. These external stressors may also increase the perceptions of the intensity of workplace stressors. Future research could help delineate the relative contribution of external stressors, workplace stressors, and a past history of MDD to the overall presence of depressive symptoms. It is noteworthy that 94% of the participants were female. It is well recognized that being female is an independent risk factor for MDD (Eid et al., 2019). In addition, Bangladeshi cultural norms include women as being responsible for meeting the care needs of all family members; thus, it is likely that many of the participants also carried additional household responsibilities related to caring for children and elderly family members. Future quantitative and qualitative studies would be useful in providing more detailed information about Bangladeshi RNs’ perceptions of work-related stressors in the context of balancing home responsibilities and workplace responsibilities. Future studies could also explore the impact of the social stigma of being a female and choosing a career as a nurse on perceptions of occupational stress.
Prior to reporting our findings from the NSS and the WCQ, it is important to address the issue of reliability, in particular as it relates to the subscales within two of the questionnaires. The overall Cronbach α scores for the NSS calculated using the included sample are similar to those calculated by other researchers who have used these scales (Alenezi et al., 2018). However, for those that reported the calculated Cronbach α scores for the subscales, there is significant variability, which raises concerns about the reliability of specific subscales and if the meaning of each subscale is perceived differently in different groups of nurses across practice settings and national and cultural contexts. Even in the original development of the NSS and its examination of its psychometric properties in a group of American nurses, Gray-Toft and Anderson (1981) reported that only four of the seven subscales had Cronbach α scores greater than .70. Subsequent articles report a wide variety of NSS subscale Cronbach α scores, most often with higher subscale scores reported in the original study. Cronbach α scores for the subscales ranging between .67 to .89 have been reported across multiple countries and practice settings (Newman et al., 2020). Other researchers only reported the overall scores (Alenezi et al., 2018) or completed principal component analysis to support the use of only the total NSS score (Mert et al., 2021). Pathak et al. (2013) suggested that factor analysis completed with the involved study sample is required to better address the differences in working conditions in LMICs. In a study with 349 nurses in Turkish and after modifying the items loading on each subscale and rewording some of the subscales, the reliability coefficients for the subscales ranged from .63 to .81 (Mert et al., 2021). Other researchers have modified the original NSS (Alkrisat & Alatrash, 2017) to better reflect hospital-based practice, to better reflect specific national context (Kim et al., 2015), or for emergency room practice (Yuwanich et al., 2018).
The calculated Cronbach α scores for the subscales in this study (Table 2) were significantly lower than reported in the above studies, which must be considered a limitation to our results. Our findings suggest that future qualitative work will be crucial to gain a better understanding of the meaning of the more common stressors that Bangladeshi nurses experience in their workplace. Using factor analysis to evaluate the Modified Nursing Stress Scale, similar to the Turkish study (Mert et al., 2021), would also be helpful for its relevance to Bangladesh.
The Cronbach α scores of the WCQ subscales were also calculated and similar to the NSS, showing some subscales with low reliability. Concerns about the reliability of the subscales are not limited to our experience. Kieffer and MacDonald (2011) completed a meta-analytic reliability generalization study and found that the Confrontive Coping and Distancing subscales generated the most variability across studies and that sample size, nature, and source of the participants, gender, and race all contributed to the observed variability. However, the authors note that the frequency of reliability reporting was less than 50%, making it difficult to draw robust conclusions. Another generalization study of the Ways of Coping found similar problems with lack of reporting reliability data in many studies but reported the subscale Self-Controlling as the most variable. The potential impact of lower subscale reliability on the results has been discussed (Labrague et al., 2018). There is also ongoing debate as to what is an acceptable reliability coefficient. Crocker and Algina (1986) suggested that, in general, 0.70 is acceptable; however, others argue a higher coefficient is necessary for confidence in the interpretation of data (Vakili & Jahangiri, 2018).
International researchers are often faced with challenging decisions at the design stage of the research process in terms of choosing well-published standardized tools. Their choices are often limited to using standardized tools, which are thought to be comparable to data from other studies, modifying tools, or having the time and skills available to develop and test a more contextually appropriate tool, which may then lack generalization. Using a standardized tool often means that it was developed in the context of a different culture, different sample, and for research with nurses working in different work environments. This study reflects our initial efforts to understand Bangladeshi RN’s workplace stressors and the potential impact on their mental health. Our choice to use standardized tools exposed significant concerns regarding the applicability of the various items within the tools to Bangladeshi RNs. However, other international researchers have also used the same instruments, which provides some measure of comparability. Thus, in this contextual frame and acknowledging the lower reliability scores in some of the subscales of both the NSS and WCQ, we discuss our findings.
The average total score on the NSS was 50.67 (SD = 11.36), similar to the total scores reported in some (Alkrisat & Alatrash, 2017) but not all studies. A study of Hong Kong surgical nurses (N=54) reported a mean total score on the NSS of 67.70 (Newman et al., 2020). Our findings that workload was the most often reported source of stress was consistent with other countries’ data (Karadzinska Bislimovska et al., 2014; Bautista et al., 2020; Newman et al., 2020). Walker et al. (2021) reported that younger nurses are more likely to feel stressed in the workplace; however, our data suggest that older, more experienced nurses can also experience significant workplace stress. Perceptions regarding workload as a stressor can include insufficient staff and/or too many non-nursing tasks as sources of workplace stress (Karadzinska Bislimovska et al., 2014). Evidence that non-nursing tasks likely account for some of the participants’ perceptions of workload as a stressor comes from the previously mentioned study that observed about 60% of Bangladeshi RNs time working within government systems was taken up with direct patient care (Joarder et al., 2021; Rony, 2021). The low nurse-to-patient ratio [2 nurses per 10,000 population] (World Health Organization, 2020) in Bangladesh may also have influenced perceptions of workload as a stressor. Based on hospital records obtained as part of the study, the hospital occupancy rate was 131.4%, and the nurse-patient ratio was 1:10 at the MCHs. Bangladesh has 76 percent of the deficit of nurses (Rony, 2021).
The other two common sources of stress identified by the RNs in the study were Death and Dying and Uncertainty regarding Treatment. All practicing nurses experience caring for terminally ill patients, rapid changes in health status, unexpected death of patients, and supporting families after the death of a loved one. These are inherently stressful events. If these essential nursing responsibilities are perceived to be affected by other workplace stressors that interfere with providing quality care for the dying patient and their families, nurses may perceive this as a chronic stressor related to system issues rather than an individual limitation. Uncertainty regarding treatment could reflect multiple circumstances, including inadequate information from physicians, unavailability of a physician when needed, uncertainty regarding how to operate specialized instruments, and concerns about the effectiveness of the prescribed treatment regime. Similar results were reported in a Macedonian study (Karadzinska Bislimovska et al., 2014).
The personal characteristics (age, marital status, professional education, and practice setting) were shown to have no significant influence on depressive symptoms, in contrast to prior studies related to age (Walker et al., 2021), professional education, or specific practice settings (Khodadadi et al., 2016). The average age and years of experience, which have multiple impacts on competence and confidence regarding workplace responsibilities, may have contributed to the observed differences in our results compared to other studies (Folkman & Lazarus, 1980).
Although personal characteristics did not influence depressive symptoms, NSS scores had a significant positive association with depressive symptoms (OR = 1.05, p < .01). This finding is in keeping with multiple other studies (Khodadadi et al., 2016; Maharaj et al., 2019). A consistent association between stress and depression has been well recognized, especially in clinical and community-based research related to sex differences in mood and anxiety symptoms and disorders (Salk et al., 2017), as well as in the literature related to occupational stress and burnout (Bianchi et al., 2015). Although the workload was shown to be the highest source of workplace stress in this study, it was not a significant predictor of depressive symptoms. Further exploration of nurses’ perceptions of their workload and their perceptions of the degree of control over their work responsibilities may help elucidate the underpinning of this apparent discrepancy.
The total mean score on the WCQ was calculated to be 52.68 (SD=17.3). Comparisons to other studies are difficult as there are multiple similar coping questionnaires, including the Ways of Coping Questionnaire (Folkman & Lazarus, 1988a) and the Ways of Coping Scale (Folkman & Lazarus, 1988b), all derived from the original tool developed by Folkman and Lazarus (1980) (Ways of Coping Checklist). In addition, in studies where participants endorsed more of the various coping strategies as described within each subscale (Al Gamal et al., 2018; Labrague et al., 2018), then the average score will be higher than reported here. In our study, the three most often used coping strategies were Seeking social support, Planful problem solving, and Positive reappraisal. Interestingly, Positive reappraisal has shown the least variability across studies (Rexrode et al., 2008), suggesting that this subscale reflects a similar meaning across populations. It is important to note that previous articles related to reliability suggest that reliability testing needs to be calculated by sex (Rexrode et al., 2008; Kato, 2015). Our sample is 94% female, thus can add to the body of knowledge regarding the impact of sex and gender on coping.
Despite any minor differences across the above-mentioned coping instruments, all share the belief as described by Lazarus and Folkman (1984), that coping involves two overarching types of strategies, actions to alter the stressor or the behavioral response or by modifying the emotions related to the internal perceptions of the stressor. Similar to our findings, previous studies reported that nurses use both types of strategies to deal with stressful situations (Ramezanli et al., 2015). Given the underlying belief about the two general styles are used with different goals in mind, direct comparisons of the average scores between the two general styles are not appropriate. Despite the original description of the two overall styles not being mutually exclusive, comparisons have been previously reported. Our finding that the overall mean score for problem-focused coping was higher than observed for emotion-focused coping was similar to some reports (Ramezanli et al., 2015). However, Jang et al. (2019) reported that emotion-focused coping scores were higher than problem-focused coping scores in a group of South Korean nurses.
The finding that both coping styles had no effect on the relationship between workplace stress and depressive symptoms was congruent with the previous study (Lin et al., 2010) but contrary to the statement of Lazarus and Folkman (1984). A possible explanation is that both types of coping styles were used by nurses to control their workplace stress. Dewe et al. (2010) revealed that both coping styles might be either detrimental or beneficial, depending on how much control an individual has over the stressful situation. Wang et al. (2011) indicated that the use of coping strategies might vary with respect to the individual, psychological, and cultural factors.
It is noteworthy that when CES-D scores were dichotomized (less than 16 and 16 or greater), we did observe group differences. There were no differences in mean scores for problem-focused coping between the two groups subdivided by CES-D scores. However, participants who scored ≥16 on the CES-D had significantly higher average scores of emotion-focused coping compared to participants with CES-D scores <16 (p= .007). Lin et al. (2010) also found there was a significant association between coping and depression.
Limitations
This study was an initial effort to increase understanding of the types of common workplace stressors experienced by Bangladeshi RNs, potential relationships among workplace stressors, depressive symptoms, and commonly used coping strategies. The cross-sectional design was appropriate at this stage, despite its limitation in terms of identifying causal relationships among relevant variables. A limitation in our study was the calculated reliability coefficients of the NSS and WCQ subscales post-data collection. From these data, part of our ongoing research plan must include exploring the meanings inherent in the various items of both tools that are specific to the context of Bangladeshi RNs and the specific workplace (MCHs), as well as the Bangladeshi health system and the more general context of Bangladeshi society. Qualitative and mixed-method research methods can make important contributions to this work. Other limitations include limiting the recruitment to RNs from government MCHs only, a single type of nurse (RNs), and in-patient practice settings, all of which may limit the generalization of the data.
Recommendations
The high incidence of CES-D score ≥ 16 indicates that a large % of RNs struggled with significant depressive symptoms. This finding could have far-reaching and rippling effects, including impacts on the status of individuals’ physical and mental health, their ability to provide quality care to their patients, their interactions with others on the health team in a positive manner, and their level of job satisfaction. Nursing education programs may need to evaluate their curriculum for current relevance. Hospital administrators may need to consider and adopt multiple strategies to address individual, systemic, and societal factors that increase job stress for Bangladeshi RNs. Such strategies as increased remuneration, increased participation in decision-making, increased personal autonomy in the workplace, specific stress management programs, advocacy at the local and national levels to increase funding to improve staff: patient ratios could all support improvements in the hospital work environment.
Conclusion
The results of this initial cross-sectional study raise serious concerns about the mental health and wellbeing of RNs in Bangladesh as it relates to various types of workplace stressors. A fuller understanding of the sources of workplace stress and the meanings attached to workplace experiences common to Bangladeshi RNs are needed as a basis to evaluate how to measure the unique sources and degree of job-related stress as experienced by RNs. Completing factor analysis on both the NSS and WCQ based on data from Bangladeshi RNs could be useful in modifying the tools for a better fit. However, our data reinforce others’ findings that measurement tools arising within developed nations may not be reliable in developing nations, which presents a significant challenge for many international researchers. Detailed narratives about the day-to-day activities that constitute RN practice in Bangladeshi MCHs would also be useful as an initial basis for comparisons across practice settings. Any improvements in the health of nursing professionals will translate to a better health care system and improvements in the quality of patient care.