









Introduction
The rapidly aging population has become an urgent global health concern (Sakakibara et al., 2015) because the long-term process of older adult care is faced with limited family and professional caregivers (Harvath et al., 2020). The widespread expectation on families, along with its ubiquity of practice to watch over their older adults, has been aligned with strong intergenerational family solidarity (Paguirigan, 2019). More so, the conception of debt of gratitude has both influenced the responsibility a significant burden. The widespread expectation in terms of family caregiving reveals that 85 to 95% of all older adults receive care from their family members on a global scale (Gaugler et al., 2018). Likewise, the need to balance personal and social roles amidst increasing pressure to provide care to an older adult becomes the caregiver’s predicament (Donovan et al., 2011; Thomas et al., 2017). Meanwhile, it gives some an opportunity to reward and fulfill role assumptions (Luichies et al., 2021; Reinhard et al., 2011).
Acceptance of caregiving roles assumption in the care for an older adult can be as sudden or carefully planned to depend on several factors. Despite the many shared experiences of family caregiving, this process varies in terms of family dynamics, nature of timing, duration, transitions of care, and end of life. Common to this journey is the acceptance of the family members to be able to enter the adjustment process of becoming their “self” in caregiving (Nguyen & Levkoff, 2020). Acceptance of change that requires family decision-making is vital to initiate action (Kristanti et al., 2021; Potter et al., 2017). Caregiving trajectory is the term used to denote the process that family caregivers undergo specifically in phases that generally include role awareness, emerging responsibilities, increasing demands for care, and finally, end of life (Committee on Family Caregiving for Older Adults; Board on Health Care Services; Health and Medicine Division; National Academies of Sciences, 2016). In the process of caregiving, acceptance and commitment as central aspects of this emerging evidence-based practice are crucial in stress levels and the quality of life of caregivers (Han et al., 2021).
Assignment of the primary caregiver for an older adult in the family is based on several factors that encompass existing relationships, gender, societal norms and expectations, geographical proximity, and moral and expected familial obligation (Luichies et al., 2021; Nguyen et al., 2021). Evidence suggests that family caregivers do not receive adequate preparation in the assumption of caregiving roles in matters related to problem-solving and communication skills (Robinson et al., 2020). Inadequate preparation and execution caused by an interplay of factors related to poor acceptance of the current condition, inadequate resources, conflict with familial and employment responsibilities and financial difficulties, and new circumstances result in inadequate adaptation to the caregiving role (Ainamani et al., 2020; Hashemi-Ghasemabadi et al., 2016; Nguyen et al., 2021). Moreover, increasing dependence on the caregiver emanates from the older adult’s functional decline over time (Ainamani et al., 2020; Pinto et al., 2021), and the caregiving role becomes more intense in the advanced and end-of-life phase (Robinson et al., 2020).
Relevant to understanding the beginning role of caregiving is acceptance of expectation. The Acceptance Theory of Family Caregiving is based on societal and familial expectations endured through several generations (Luichies et al., 2021). In simpler terms, the family caregiver is aware of such a responsibility of looking after the older adult when the time of physical and cognitive decline and dependency emerge while it is also an expectation of the older adult to have someone to look after them when the time comes amidst the possibility of embarrassment or perceived burden on family caregivers (Bekhet & Garnier-Villarreal, 2020; Hickman et al., 2020; Kellner et al., 2017). Therefore, a successful view on adaptation to family caregiving roles prerequisites acceptance.
While cultural expectations on family caregiving hold true, it is vital to determine the degree of family members’ acceptance as it is integrated within them. Therefore, this study aims to develop a theory that explains the acceptance of caregiving roles by the family caregiver for the older adults necessary to predict behavioral adaptation and control caring phenomenon that favors successful meeting of caring expectation across trajectory phases and transitions. Developing a working knowledge of acceptance as it vitally influences caring behaviors among family caregivers contributes to older adults’ health and well-being. Imperative to this understanding shall be beneficial in relating it with family caregivers’ preparedness, self-efficacy, and quality of life secondary to planned behavior of caring.
Methods
The Acceptance Theory of Family Caregiving utilized a deductive approach. Starting with broad concepts and determining which concepts apply to populations, the top-down approach leads to the formulation of conclusions, known as deductions. For a sound deduction to occur, generalizations must be true because this is where logical consequences can be drawn (Utley et al., 2017). As a premise for deductive argument, an axiom is a logical principle assumed to be true and chosen carefully to avoid inconsistency. Axioms demonstrate consistency, plausibility, and richness to provide a system of logic in the creation of a theory. From a generalized statement that contains abstractions, a theory explains and predicts the interrelationship of variables through its ideas, concepts, and themes (Kivunja, 2018).
With the use of a deductive method to theory development, generalizations about the caregiving process, family psychology, cultural influence of older adult care, and gerontology nursing were determined through rigorous literature reviews. The definition of a family caregiver applies to any relative, partner, friend, or neighbor of the older adult that is based on a significant relationship. Following a literature review, the iterative yet sequential process of searching, screening, and assessing related works proceeded with data extraction and analysis (Paré & Kitsiou, 2017). Data extraction and analysis resulted in the identification of trends and patterns to systematically view the statements that were generally accepted to be true. These non-debatable facts known as axioms were identified, which subsequently became the basis for propositions. An axiomatic approach paved the way for preserving and furthering the growth of the discipline that tackles older adult care through family caregiving. Building the theory through logic and axiomatic systems of the behavior (Levy, 2017) of family caregiving, identification of propositions from the theory, and establishing testable hypotheses are placed at the process.
The proposed Acceptance Theory of Family Caregiving is an example of a mid-range theory that describes, explains, and predicts phenomena of caregiving of older adults by the family members in the practice of gerontology nursing. It also describes how the variables, namely acceptance, the trajectory of caregiving, resources, and cultural influence, relate with each other.
Results
Consistent with the deductive axiomatic approach to theory generation, literature reviews play a crucial role in the identification and support of the identified axioms and propositions in the buildup of the theory. Table 1 illustrates the extracted four axioms that were derived from literature reviews, and these served as the reference in the formulation of four propositions necessary in the framework of the developed acceptance theory of family caregiving.
| Axioms | Propositions | Theory |
|---|---|---|
|
Axiom 1 Family relationships are founded based on commitment derived from various forms. |
Proposition 1 Older adults who expect their children to take care of them as they age have cultural influence. |
Care of the older adult in the family caregiving process is determined by the acceptance of role assumption by the family caregiver across trajectory phases (Acceptance Theory of Family Caregiving) |
|
Axiom 2 Acceptance pre-requisites successful adaptation to one's environment. |
Proposition 2 Acceptance of the role will determine the caregiver’s acceptance of consequences in the form of physical, economical, psychological, and spiritual aspects. |
|
|
Axiom 3 Acceptance of the caregiving role is a process. |
Proposition 3 Family members who accept the possibility of the decline of their older adults are more likely to be prepared to assume caregiving roles. |
|
|
Axiom 4 The family, as a unit, strives for balance and requires resources to sustain it. |
Proposition 4 The trajectory family caregiving process is influenced by factors such as resources. |
The role of a significant relationship between older adults and that of the family caregiver extends beyond influences of blood and marriage through the commitment of various forms explicitly referred on the definition of family caregiver that refers to any relative, partner, friend, or neighbor who provides a broad range of assistance-related activities with a basis of significant relationship to an older adult with chronic and disabling conditions. Therefore, family relationships are founded based on commitment derived from various forms (Axiom 1), which implicates those older adults who expect their children to take care of them as they age have cultural influence (Proposition 1).
Acceptance of the change is crucial to successfully adapt to family dynamics, atmosphere, and role assignments in the presence of older adults that require family caregiving. While it explains that acceptance pre-requisites successful adaptation to one’s environment (Axiom 2), the beginning and unfolding responsibilities demand careful family discussion in addressing the older adults’ needs along with the caregiver responsibilities that accompany them along with all phases of family caregiving trajectory, thereby suggests that acceptance of the caregiving role is a process (Axiom 3). The widespread expectation of pursuing caregiving of the older adults supports the idea that acceptance of the role will determine the caregiver’s acceptance of consequences in the form of physical, economical, psychological, and spiritual aspects (Proposition 2). Furthermore, the acceptance of role is challenged as responsibilities of family caregiving unfold that may present role ambiguity, future uncertainty, and self-efficacy concerns during care provision. This implies that whatever change the older adults present during the term of care provision, the family caregiver is ready to accept the consequences that may accompany role assumption supporting the idea that family members who accept the possibility of the decline of their older adults are likely to be prepared to assume caregiving roles (Proposition 3).
Following unfolding responsibility in the family caregiving trajectory, increasing care demands lead to surrogacy in terms of healthcare decisions and physical care. This is congruent with the idea that the family, as a unit, strives for balance and requires resources to sustain it (Axiom 4). Therefore, the trajectory family caregiving process is influenced by factors such as resources (Proposition 4). Acceptance of the caregiving role also means that end-of-life care terminates the family caregiving trajectory. This requires more intensive caregiving demands, which supports that acceptance of the role will determine the caregiver’s acceptance of consequences in the form of physical, economical, psychological, and spiritual aspects (Proposition 2). This idea is applied not only in the final phase of the family caregiving trajectory but is also evident during unfolding responsibilities and increasing care demands.
Discussion
Literature postulates the dynamism of family relationships as crucial to understanding the behavior of its members. Children and parents, for instance, remain closely related across the course of life, and the well-being of these individuals is guaranteed by the quality of intergenerational relationships that they have. These relationships are enduring and consequential, and their behavior is a result of the years they have been together (Schulz et al., 2020; Thomas et al., 2017). The quality of family relationships in the form of support and supervision determines the favorable influence and consequently acceptance among growing children of the responsibility that they hold as their older adults age. Children of the older adults, for instance, assume roles from a personal perspective with the basis of obtaining profound meaning and reward and as a means of giving back the love and care they were given as children along with the idea that central to their well-being is the commitment to favor connection of generations (Reinhard et al., 2011; Thomas et al., 2017).
Shared within the context of familial relationships and rearing, beliefs that underpin the family members’ behavior in the care of their older adults encompass culture (Revenson et al., 2016). Who ends up as becoming the primary caregiver is shaped by existing relationships to the older adult in need of care, gender expectations, cultural background, and geographic proximity (Scheibl et al., 2019; Solomon et al., 2018). Primary caregivers may range from a spouse or any other family members, and this decision is determined by cultural factors (Donovan et al., 2011). Family caregivers often serve as advocates and coordinators of care, and their roles are unfolded within transitions of caregiving trajectory. Assumption of caregiving roles by the family member is directed towards achieving a satisfactory level of acceptance regarding this crucial decision-making process which is highly influenced by widespread cultural expectation (Committee on Family Caregiving for Older Adults; Board on Health Care Services; Health and Medicine Division; National Academies of Sciences, 2016; Reinhard et al., 2011). The cultural influence of both the older adults and the caregivers likewise provides direction in the choice of culturally appropriate care that the recipient requires. This likewise connotes that caregiving services become highly individualized for the older adults to receive compared to when they are delivered by service agencies, implicating the cultural relevance of family caregiving societal acceptance (Donovan et al., 2011; Revenson et al., 2016). Endured by generations, the witnessed caring practices have somehow shaped the family members’ views of anticipating the care of the older adults in the future. It is also grounded from the influences of internalized debt of gratitude and desire to give back the care they once received, thereby enhancing their motivation to accept family caregiving roles.
Equally important in exploring the cultural and relationship-based nature of the concept of family caregiving is the understanding of the process to denote when it begins, pursues, and terminates. The trajectory of family caregiving begins with the awareness of the family members towards the older adults’ behavioral indication or changes in health that may warrant a certain degree of caregiving (Gilbert et al., 2018). Functional impairment, when gradually observed, provides subtle assumption of acceptance of family caregiving as compared with sudden older adult’s health decline that proves challenging (Committee on Family Caregiving for Older Adults; Board on Health Care Services; Health and Medicine Division; National Academies of Sciences, 2016). The Roy Adaptation Model explains the interaction of a person in a changing environment (Ursavas et al., 2014). Given the complexity of family caregiving, preparedness for the responsibility is crucial. Inadequate preparation of the caregivers is what constitutes burnout (Committee on Family Caregiving for Older Adults; Board on Health Care Services; Health and Medicine Division; National Academies of Sciences, 2016). This denotes the relative importance of acceptance as a requirement for being prepared to assume caregiving roles. While the intensity of required assistance may not be as exhausting in the initial phase of the caregiving trajectory, accepting the role prepares the caregiver for more challenging roles in the future. The psychological well-being of the family caregiver relates to acceptance of the role that positively influences the outcomes of the caregiving (OMalley & Qualls, 2020). Studies pointed out higher anxiety levels and burden caused by longer duration of caregiving, which can be attributed to required duties that range from provision of assistance to direct administration of services to the care recipient, assistance with household activities, self-care measures, ambulation or mobility, emotional and social support provision, advocacy, coordination of required health care and surrogacy (Committee on Family Caregiving for Older Adults; Board on Health Care Services; Health and Medicine Division; National Academies of Sciences, 2016; Lou et al., 2015). The need to balance personal and social roles in these trying times can prove to be challenging, specifically with respect to competing pressures of employment, watching over their own children, and older adult care (Donovan et al., 2011; Thomas et al., 2017). The widespread expectation of pursuing caregiving of the older adults provides clear implications that informal caregiving is what families must take as a primary responsibility (Revenson et al., 2016).
The unpredictability of the older adult’s condition and poor acceptance of role compromise the process of caregiving, leading to disadvantaged positions for both parties (Camak, 2015; Committee on Family Caregiving for Older Adults; Board on Health Care Services; Health and Medicine Division; National Academies of Sciences, 2016). Over time, the older adult’s dependency contributes to increasing reliance on the family caregiver to perform required functions (Schulz et al., 2020). Consequently, the caregiver is expected to provide more assistance than usual which compromises resources and work-life balance. Change in caring status and demands results in strengthening coping secondary to required adaptation. While increasing physical dependence leads to more caregiving demands, there is not always a negative consequence as some family caregivers find fulfillment in the accepted caring roles. Domains of care may include monitoring older adults’ condition, medication administration, communication with healthcare professionals, and transition from home to hospital or facility management. This implicates that family caregivers are introduced as partners with healthcare professionals in the integration of a collaborative approach of care with an emphasis on caregiver-friendly policies and flexible arrangements (Bell et al., 2019). On a similar note, better transitional care calls for effective and quality care as the transition from one setting to another proves to be the most vulnerable and traumatic experience of the family caregiving process (Reinhard et al., 2011).
Caregiving roles may change over time and may be highly individualized as older adults tend to go into the transition from one health care setting to the other, changes in the familial, social, and geographical context of care provision. While transitions can be planned as in the case of scheduled older adult’s follow up in the hospital or unplanned such as emergency room visit or required re-admission, that certain degree of unpredictability of family caregiving proves that the family members’ needs and dynamics must be assessed periodically so that their needs are addressed during transitional periods (Committee on Family Caregiving for Older Adults; Board on Health Care Services; Health and Medicine Division; National Academies of Sciences, 2016; Gitlin, 2019). Caregiving responsibilities are considered acute for families if older adults suffer from abruptly appearing conditions such as stroke, dementia, or even mental illness (Gitlin, 2019). These often become troublesome as the older adult’s condition becomes complex and their behaviors become severe (Liu et al., 2018; Reinhard et al., 2011). Acceptance of the nature of predictability of the older adult’s condition over time makes caregiving roles well-tolerated alongside the idea that family members are more likely equipped to respond to demands when prompted.
The increasing complexity and intensity of older adults’ conditions prove to be challenging as they are burdened by their decisions to determine what would be best for their older adults (Jehangir et al., 2019; Reinhard et al., 2011). With respect to the beginning and sustaining family caregiving process, caregivers relied on siblings and other support services to communicate older adults’ intensified needs (Gilbert et al., 2018). Monetary resources to pave the way for medication procurement, check-up, and required to follow up are crucial to both the health of the family caregiver and older adult (Committee on Family Caregiving for Older Adults; Board on Health Care Services; Health and Medicine Division; National Academies of Sciences, 2016). The amount and type of care the family caregivers provide heavily depends on economic resources and the demand for the family caregiver’s time and energy (Kaplan & Berkman, 2021; Schulz et al., 2020). Despite challenges, caregivers find meaning and purpose at the end-of-life care phase of family caregiving (Committee on Family Caregiving for Older Adults; Board on Health Care Services; Health and Medicine Division; National Academies of Sciences, 2016; OMalley & Qualls, 2020). The cultural beliefs that underlie the older adults and the family caregivers are crucial to care provision in this process (Revenson et al., 2016).
With an unprecedented demographic imperative of the global population of older adults, specific family caregiving implications arise (Gitlin, 2019). The concepts related to family caregiving encompass the phenomenon as a process influenced by resources, cultural expectation, and degree of acceptance by caregivers who provide care to an older family member. The development of a theory to fully understand this process is beneficial to certain degrees as it explains the occurrence of practice, predicts based on future empirical evidence, and controls the process that favors both the older adult and the caregiver. This theory can greatly contribute to the practice of gerontology nursing in matters relating to older adults’ health and well-being, family structures and relationships, and caregiver self-efficacy and fulfillment. As the family caregivers represent the health care system’s partners to ensure older adults’ maximal health, understanding this theory from the perspective of both the older adults and their caregivers is essential.
The Acceptance Theory of Family Caregiving aims to explain acceptance as vital in the trajectory phases of caregiving, not only on the older adult but also on the family caregiver to initiate needed actions (Potter et al., 2017). It also aims to predict that inadequate preparation to caregiving role assumption due to poor acceptance of the demanded situation often leads to caregiver burden (Committee on Family Caregiving for Older Adults; Board on Health Care Services; Health and Medicine Division; National Academies of Sciences, 2016). Therefore, mitigation strategies to address caregiver burden is to allow the family caregivers to realize the change that demands adaptation, and only through acceptance of family caregiving role should adjustment set in (Nguyen & Levkoff, 2020).
Within the bounds of familial relationships and widespread cultural expectation, the care of the older adults translates as a responsibility of the family members endured by several generations (Gaugler et al., 2018). The strong inter-generational solidarity emphasizes that family caregiving, as the name implies, is based on a commitment derived from cultural and familial factors (Paguirigan, 2019). Varying from these influences, the family caregiving process, known as trajectory, involves a series of phases that present several challenges to both older adults and family caregivers (Committee on Family Caregiving for Older Adults; Board on Health Care Services; Health and Medicine Division; National Academies of Sciences, 2016). Requisites to meeting each phase of the process is a degree of acceptance of role assumption by the caregiver that equates to the anticipation of the requirement of resources, role changes, and demands with respect to awareness, unfolding responsibilities, increasing demands, and end of life phases of family caregiving.
Acceptance Theory of Family Caregiving
Understanding acceptance also intends to communicate it as inherent in family relationships within the context of older adult care (Schulz et al., 2020; Thomas et al., 2017). While it is an expectation for older adults to have someone to care for them when dependency calls for caregiving roles, the crucial role it plays determines the success of the family caregiving process (Luichies et al., 2021). At some point in their lives, older adults require someone to perform for them the activities of daily living owing to increasing physical dependency and cognitive decline. The acceptance of a family member’s caregiving role, while a process, is situated in every phase of the family caregiving trajectory. Associated with motivation, acceptance is a driving mechanism that influences the behavior of the family caregiver in performing roles that are unique in every step of caregiving.
Figure 1 shows the theory’s framework as it relates to the essential concepts of family caregiving. Central to the framework is acceptance infused within the overlapping trajectory phases: awareness, unfolding responsibilities, increasing care demands, and end of life. The diagram attempts to communicate that as the phase/s (represented by green circles) move away from acceptance (represented by a yellow circle), it decreases infusion not only with acceptance but successful family caregiving (represented as a large red circle) as well.
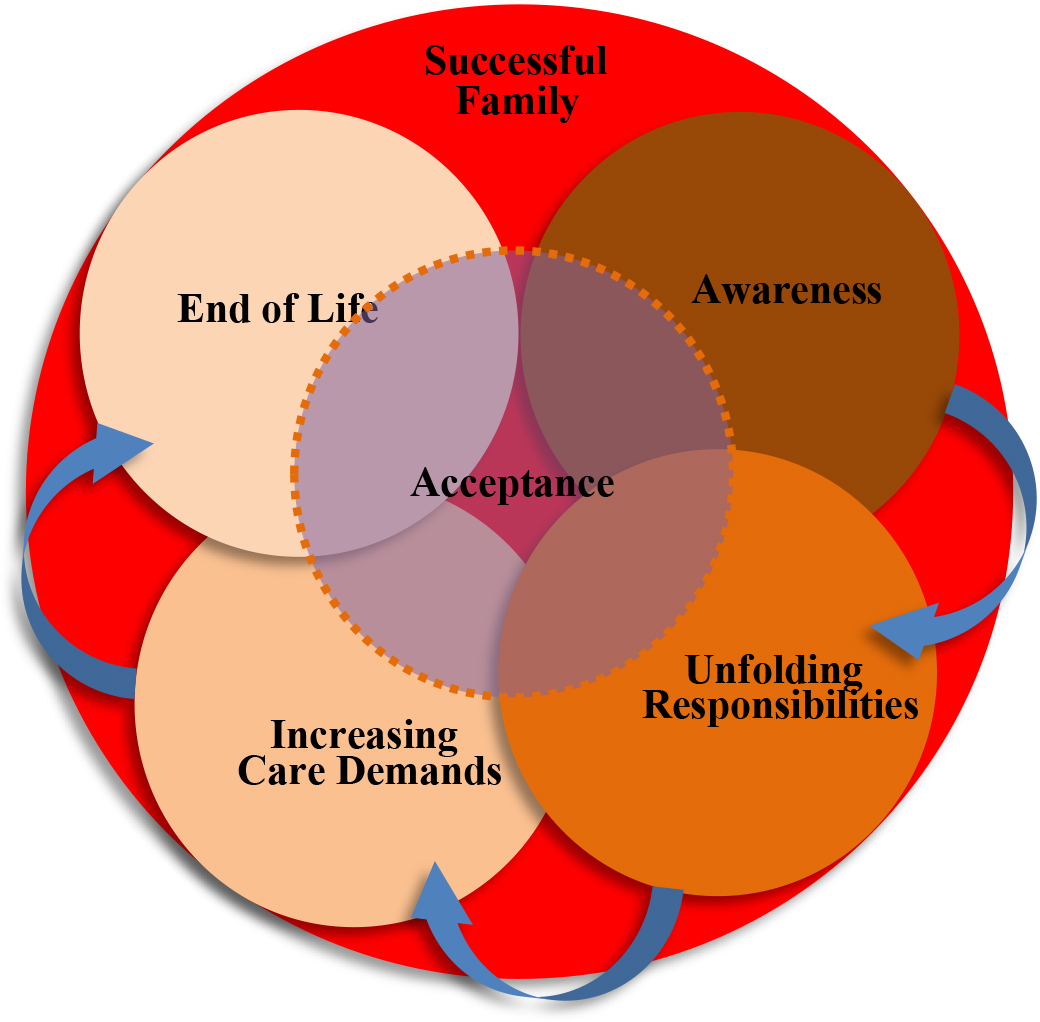
The overlapping trajectory phases imply the stages that every family caregiver goes through with respect to the needed assistance of the older adult. As the care can be highly individualized, the demands vary along with other determinants, including resources and self-efficacy. Similarly, there is a variation in terms of the duration by which the family caregiver undergoes, along with the gradual or sudden emergence of care demands. The care of the older adult in the family caregiving process is determined by the acceptance of role assumption by the family caregiver across trajectory phases, crucial in the understanding of successful family caregiving.
The theory is applied among families whose care of older adults is within their domain. It may not be fully applied to families that delegate the care of their older adults in nursing facilities. In addition, the underlying cultural acceptance of family caregiving influences the theory’s applicability. Lastly, the definition of the family caregiver in the context of this theory extends beyond the influence of blood and marriage, consistent with related literature and studies. Going through the provided definition minimizes confusion relating to the population scoped within the theory.
Conclusion
While several challenges await the family caregiver in the assumption of societal and culture-based measures alongside the expectation of older adult care, much concern is concentrated on their health status over the caregiver’s situation. The discrepancy of the care recipient and provider focus paved the way for a developed theory that targets acceptance of these challenging roles of the provider as it greatly determines the outcomes of favorable healthcare outcomes of the recipient. The developed theory suggests that the care of the older adult in the family caregiving process is determined by the acceptance of role assumption by the family caregiver across trajectory phases. This study highlights the vital implication of acceptance of role assumption to the outcomes of the caregiving process with respect to older adult care, prevention of family caregiver burden, and establishment of strong familial and social relationships.