









Background
The number of aging persons has been increasing dramatically worldwide over the past few decades (Feliciano et al., 2022). The aging population is linked to an increased burden of non-communicable disease disorders, all-function organ dysfunction (Amarya et al., 2018), poor health status (McPake & Mahal, 2017), and complex medical needs (Chandra et al., 2015), which necessitate long-term care (McPake & Mahal, 2017). Age, functioning, polypharmacy, pharmacotherapy complexity, inappropriate drugs used for older persons, and multimorbidity contribute to the high demand for care. Return visits to the Emergency Department (ED) following hospital discharge can be linked to such factors (Deschodt et al., 2015; Naseer et al., 2020; Salvi et al., 2017; Schoonover et al., 2014).
ED visits are common among older adults (Pham et al., 2009). Previous research has shown that 10-26 percent of older persons attend the emergency room (de Gelder et al., 2018; Lowthian et al., 2016). Aging patients made more than five ED visits per year, accounting for 15% of all visits (Ukkonen et al., 2019). Furthermore, dyspnea from COPD was the most common chief complaint expressed by the elderly with disease-related visits to the ED (Paksopis et al., 2019; Song et al., 2016). A previous study reported that nearly 55.2 percent of all ED visits were older adults with COPD (Hasegawa et al., 2014). A high rate of visiting ED among persons with COPD occurred after hospital discharge, mostly due to the symptom exacerbation (Paksopis et al., 2019; Song et al., 2016). Therefore, it is necessary to prevent acute exacerbation in COPD patients at home, which requires transitional care to treat and stabilize patients’ symptoms to return to their normal lives outside the hospital. Optimal transitional care from hospital to home in aged care is quality in health care standards and indicators as recommended in the research field of transitional care (Allen et al., 2014). Additionally, the use of emergency services after being discharged from the hospital can be a predictor that the transitional care process is inadequate (Santos et al., 2019).
Transitional care is a broad term for medical approaches that facilitate the safe and timely transition of elderly patients across care levels and settings (Naylor & Keating, 2008) from pre-hospital discharge and prompt follow-up following hospital discharge (Naylor et al., 2011). Transitional care for elderly patients is essential to minimize medication errors, adverse drug events, lack of timely follow-up care management, and unnecessary ED visits (Kessler et al., 2013). In addition, transitional care is required to avoid discontinuity of treatment and adverse effects on older patients. On the other hand, the poor transitional care led to increased emergency treatment (Son & You, 2015). Therefore, Transitional Care Interventions (TCIs) in the older population are interesting to prevent adverse events during the transition and reduce ED visits.
Few systematic reviews of studies are available on what is the best transitional care intervention to reduce ED visits in older individuals. In 2020, similar research released a systematic review on the impact of transitional care interventions on hospital readmissions in elderly medical patients (Rasmussen et al., 2021). However, the study’s primary outcome is hospital readmission, and the findings are equivocal, indicating that there is no evidence to advocate a specific intervention. As a result, more knowledge on interventions that minimize ED visits by older adults is needed to help health care workers, particularly nurses, identify and implement effective transitional care interventions to reduce the ED visit in these populations.
Methods
Design
A systematic review design was employed. Prior to data collection, this review was entered into the PROSPERO database (CRD42021261326). It follows the Preferred Reporting Items for Systematic Reviews and Meta-Analyses guidelines (PRISMA).
Eligibility Criteria
Studies that focused on interventions towards older adult patients were considered. All studies, including older adults discharged from a general medical ward or emergency department using the PICO framework, were included (Table 1). In addition, interventions aimed at people in the transitional phase were studied, and the impact on ED visits was calculated. The interventions were required to involve either pre-or postdischarge components by either the provider or the patient management, with the number of ED visits being the primary measure. Randomized controlled trials (RCTs), quasi-experimental designs, retrospective studies, cohort studies, and case-controlled studies were required. Studies were omitted if the target population was under 60 years old or if the result was not an ED visit.
| PICO format | |
| Population | Older patients |
| Intervention | Transitional care interventions |
| Comparison | Usual care |
| Outcomes | ED visits |
Data Sources
From January 2011 to August 2021, this study examined the following bibliographic databases to find relevant studies: PubMed, The Cochrane Library, Cumulative Index to Nursing and Allied Health Literature (CINAHL), Web of Science, ProQuest, and The JAMA Network.
Search Strategy
Only studies in English published during the year 2011-2021 were included in the searches. The bibliographic searches took place between 15 July and 6 August 2021. Searching terms applied to search articles were based on MESH terms “transitional care, discharged intervention, emergency room visit, older adults”. Keyword and inclusion criteria used for searching in each database are shown in Table 2.
| Databases | Main search | Limit | Search found (N) | Meet criteria (N) | Reasons for exclusion |
|---|---|---|---|---|---|
| ProQuest | (“transitional care” OR “discharge planning”) AND (“intervention”) AND (“emergency department visit” OR “emergency room visit”) AND (“older adults” OR “elderly “OR “aged”) |
|
869 | 22 | Outcome and population are not matched; not intervention studies; not transitional care interventions; systematic review |
| CINAHL | (“transitional care” OR “care transition” OR “discharge planning”) AND (“intervention” OR “program”) AND (“emergency department visit” OR “emergency room visit”) AND (“older adults” OR “elderly” OR “geriatrics” OR “aging” OR “aged ”) |
|
135 | 16 | The outcome is not matched; not intervention studies |
| Web of Science | (“transitional care” OR “discharge planning”) AND (“intervention” OR “program”) AND (“emergency department visit” OR “emergency room visit”) AND (“older adults” OR “elderly” OR “geriatrics” OR “aging” OR “aged”) |
|
61 | 14 | Not transitional care interventions; outcome is not matched; not intervention studies |
| PubMed | (“transitional care”) OR (“transition of care”) OR (“discharge planning”) AND (“intervention” OR “program”) AND (“emergency department visit”) OR (“emergency room visit”) OR (“emergency department attendance”) OR (“emergency room attendance”) AND (“older adults”) OR (“elderly”) OR (“geriatrics”) OR (“aging”) OR (“aged ”) |
|
127 | 15 | The outcome is not matched |
| The Cochrane Library | (“transitional care” OR “discharge planning”) AND (“intervention”) AND (“emergency department visit” OR “emergency room visit”) AND (“older adults” OR “elderly”) |
|
34 | 3 | The outcome is not matched; not transitional care interventions |
| The JAMA Network | (“transitional care” OR “discharge planning”) AND (“intervention” OR “program” OR “strategies”) AND (“emergency department visit” OR “emergency room visit”) AND (“older adults” OR “elderly”) |
|
60 | 4 | The outcome is not matched; not transitional care interventions |
Study Selection
First, the first author assessed titles for their possible relevance to the population and outcome (LJ). Second, two authors independently reviewed titles and abstracts to see if they were intervention-worthy (LJ and PS). Third, two authors separately assessed the entire material. In the event of a disagreement, a third author (WS) was validated and discussed.
Quality Appraisal
The Joanna Briggs Institute (JBI)’s critical appraisal techniques were used to evaluate the trustworthiness, relevance, and findings of published publications (Joanna Briggs Institute, 2020).
Data Extraction
The Cochrane Data Extraction Form was altered to accommodate the current patient group and intervention type (Cochrane, 2022). Two researchers independently extracted data from the listed studies. Author, year of publication, nation, study design, setting, participants, study size, outcomes, follow-up period, and impact of intervention in numbers and/or percent were among the study features and results extracted. Only information about the ‘ED visit’ outcome was extracted and evaluated.
Assessment of Risk of Bias
Two reviewers (LJ and PS) separately rated the methodological quality. The papers were assessed using the risk of bias criteria according to Cochrane Effective Practice and Organisation of Care (EPOC) (2017). Allocation sequence generation, concealment of allocation, similar baseline outcome measurements, similar baseline characteristics, incomplete outcome data, participant blinding, outcome assessor blinding, contamination protection, selective outcome reporting, and other potential sources of bias in studies were evaluated by two reviewers. Validation and determination of whether the requirements were completed were done through discussion or consultation with a third researcher (WS). According to Davey et al. (2013), reviewers classified each study as ‘Low’ if all criteria were rated as ‘Low risk,’ ‘Moderate’ if one or two criteria were rated as ‘Unclear’ or ‘High risk,’ and ‘High’ if more than two criteria were rated as ‘Unclear’ or ‘High risk’.
Data Synthesis and Analysis
Methodological quality, intervention characteristics, outcomes, statistical significance, and the direction of observed effects were all used to characterize the research findings. One primary reviewer (LJ) reviewed each study and recorded all of the characteristics of the therapy investigated. Individual research was looked at further to check if they utilized the same or different terminology to describe the same elements. A set of core elements was created as a result of this method. After then, each individual intervention was evaluated once more to see if it fit into one of the categories or not. The prior processes were double-checked by a second reviewer (PS), who was a student’s supervisor. Summaries of intervention effects were computed for each trial, when possible, using risk ratios (RR) for binary outcomes and standardized mean differences (SMD) for continuous outcomes. This review attempts to do meta-analyses to determine the effectiveness of transitional care intervention by using RevMan V 5.4.1 software (https://training.cochrane.org/online-learning/core-software-cochrane-reviews/revman/revman-5-download/download-and-installation). The meta-analysis process could not be completed because the included studies had poor methodological studies, discrepancies in follow-up measure-ment, and multi-component characteristics of the intervention.
Results
Study Selection
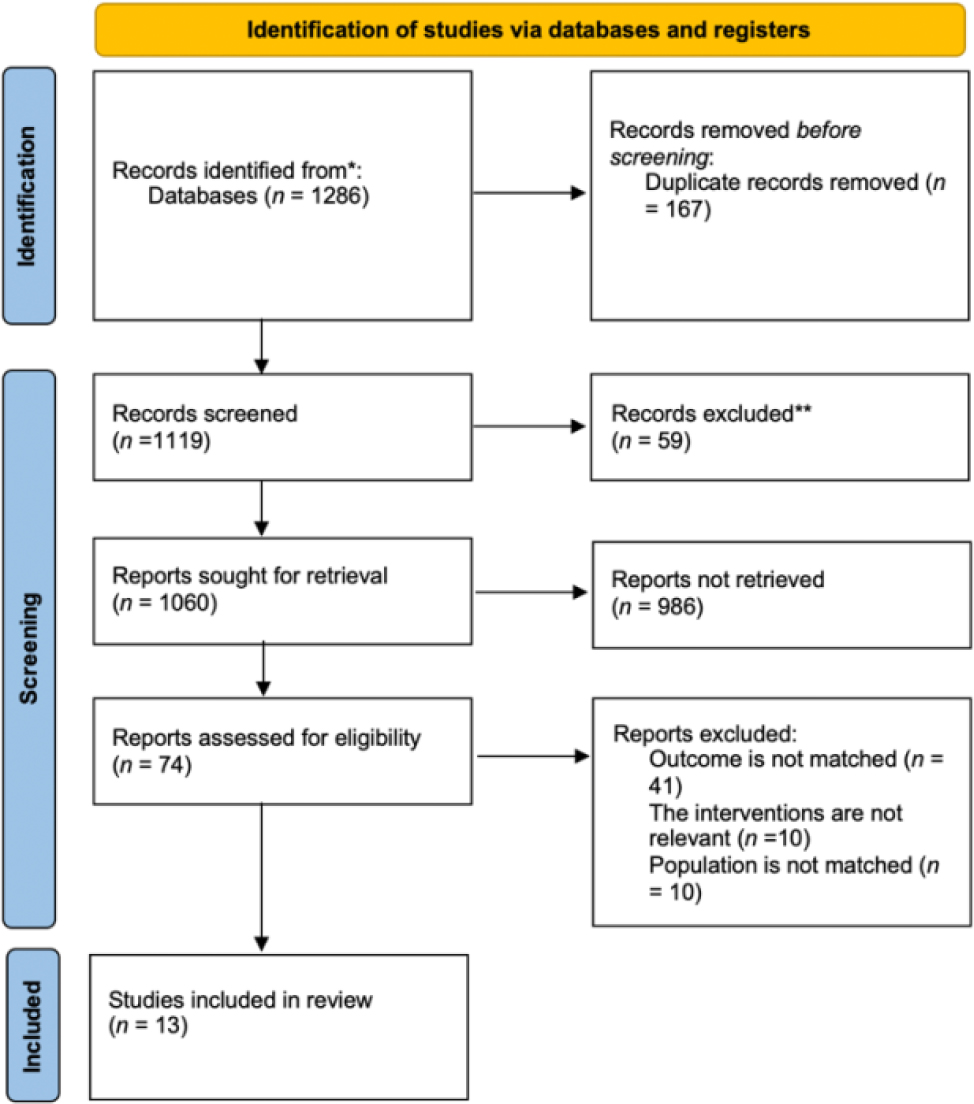
A total of 1152 records were found, and 1085 records were screened by title and abstract after duplicates were removed. A total of 59 records were examined for full-text review, with 13 meeting the eligibility requirements. Participants’ age, population, research design, or ED visit were not reported as outcomes in the 46 remaining entries, as shown in Figure 1.
Study Characteristics
The 13 trials included in the study contained 13 different therapies and outcome evaluations that measured ED visits at various time intervals. Table 3 lists the study’s features. Six of the studies included were RCTs (Enguidanos et al., 2012; Legrain et al., 2011; Liang et al., 2021; Mi et al., 2018; Occelli et al., 2016; Schapira et al., 2021), four were non-randomized controlled trials (NRCTs) (Heeren et al., 2019; Lee et al., 2018; Low et al., 2015; Robinson et al., 2021) and three were retrospective studies (Kim et al., 2021; Sabir et al., 2019; Wee et al., 2014). Individual study sample sizes ranged from 199 to 4835 people. Within 1–12 months of discharge, outcome evaluations were undertaken. Aside from ED visits, the 13 studies looked at hospital readmission (Heeren et al., 2019; Kim et al., 2021; Liang et al., 2021; Low et al., 2015; Sabir et al., 2019; Schapira et al., 2021; Wee et al., 2014), the mortality rate (Enguidanos et al., 2012; Heeren et al., 2019; Liang et al., 2021), functional decline (Heeren et al., 2019), health outcome (Lee et al., 2018), the impact of polypharmacy (Sabir et al., 2019), health care cost (Kim et al., 2021), self-efficacy (Enguidanos et al., 2012), and patient’s satisfaction (Enguidanos et al., 2012). Three studies were carried out in the United States (Enguidanos et al., 2012; Kim et al., 2021; Mi et al., 2018), two in France (Legrain et al., 2011; Occelli et al., 2016), two in Singapore (Low et al., 2015; Wee et al., 2014), one in Argentina (Schapira et al., 2021), one in the New Zealand (Robinson et al., 2021), one in Belgium (Heeren et al., 2019), one in the Hongkong (Lee et al., 2018), one in the UK (Sabir et al., 2019), and one in Taiwan (Liang et al., 2021). Between 2011 and 2021, the research was published.
| Author (year) | Country setting | Design | Intervention | Study population | Outcomes | ED visit measured time | ED visit rate (IG) | ED visit rate (CG) | RR/OR (95%CI) |
|---|---|---|---|---|---|---|---|---|---|
| Schapira et al. (2021) | A tertiary care university hospital, Buenos Aires, Argentina | Single-blinded RCT |
Predischarge: 1. A comprehensive geriatric assessment 2. Tailored recommendation 3. Transition of care Postdischarge: 1. A health and social care counselor |
Adults > 75 Total 240 (IG=120, CG=120) |
Hospital readmission; ED visit; Mortality rate |
6 months after D/C |
N = 120 n = 52 43.3% |
N = 120 n = 72 60% |
RR = 0.722 (0.562-0.929) |
| Robinson et al. (2021) | Auckland, New Zealand | A non-RCT |
Predischarge: 1. A comprehensive geriatric assessment 2. Transition of care 3. Care planning 4. Self-management education Postdischarge: 1. Follow-ups |
People aged >75 IG =1085 CG = 3750 |
ED visit; Mortality rate |
12 months after D/C |
N = 1085 n = 56 0.05% |
N = 3750 n = 420 0.11% |
OR = -0.07 (-0.10-0.04) p <0.001 |
| Low et al. (2015) | Largest tertiary hospital, Singapore | A quasi-experimental study using a pre-post design |
Predischarge: 1. Care plan Postdischarge: 1. Care plan 2. A comprehensive need assessment |
259 elderly aged> 60 years | Hospital readmission; ED visit |
3 months after D/C 6 months after D/C |
N = 259 Pre 410 Post 217 47.1% reduction N = 259 Pre 625 Post 324 48.2% reduction |
- | NR |
| Heeren et al. (2019) | University Hospitals, Leuven, Belgium | A quasi-experimental study (sequential design with two cohorts) |
Predischarge: 1. Care plan Postdischarge: 2. Follow-ups |
Patients aged >70 years CG=768 IG= 857 |
ED visits; hospitalization rate; functional decline; and mortality. |
1 month after D/C 3 months after D/C |
N = 857 n = 112 13.1% N = 857 n = 205 23.9% |
N = 768 n = 93 12.1% N = 768 n = 170 22.1% |
NR |
| Lee et al. (2018) | A community in Hong Kong | A matched-control quasi-experimental design |
Postdischarge: 1. Rehabilitation 2. Cognitive and memory training |
122 pairs of older adults and their caregivers | Health outcome; ED visits |
3 months after D/C 6 months after D/C |
N = 61 -0.66 ±1.03 N = 61 -0.49 ±0.96 |
N = 61 0.05 ±0.76 N = 61 0.07 ±0.68 |
NR |
| Sabir et al. (2019) | Leeds Teaching Hospitals NHS Trust (LTHT), UK |
Retrospectvely collected |
Predischarge: 1. A patient information leaflet and a web-page Postdischarge: 1. Refer information/ an outcome to a community pharmacist |
621 patients aged 65 and over | Hospital readmission; ED visit; Impact of polypharmacy |
6 months prior to D/C 6 months after D/C |
N = 621 Pre 214 34.13% Post 171 27.27% |
NC | NR |
| Liang et al. (2021) | National Yang-Ming University Hospital, Taiwan | RCT |
Predischarge: 1. Provided wireless transmission devices Postdischarge: 1. Telemonitoring through wireless transmission devices 2. Home visit |
IG = 100 CG= 100 |
Hospital readmission; ED visit; Mortality rate |
6 months after D/C |
N = 100 n = 12 12% |
N = 100 n = 26 26% |
OR =0.388 (0.183-0.822) P = 0.013 |
| Kim et al. (2021) | A primary care internal medicine residency clinic, USA | Retrospective study |
Predischarge: 1. Medication counseling Postdischarge: 1. Phone visit 2. Face to face teach back 3. Health education |
65 older patients | Hospitalization; ED visits; Health care cost |
1 month after D/C 2 months after D/C 3 months after D/C 6 months after D/C |
N = 49 n = 2 n = 2 n = 6 n = 25 |
N = 52 n = 12 n = 10 n = 17 n = 40 |
NR |
| Enguidanos et al. (2012) | USA | RCT |
Postdischarge: 1. Home visit 2. Phone call visit |
Older adults (N = 199) | Self-efficacy; Patient’s satisfaction; ED visit |
6 months after D/C |
N = 100 n = 0.5 1.2% |
N = 99 n = 0.99 2.5% |
NR |
| Legrain et al. (2011) | Six acute geriatric units (AGUs) in Paris and its surroundings. | Open-label, six-month prospective, randomized (Zelen design), parallel-group trial |
Predischarge: 1. Comprehensive chronic medication review 2. Self-management education 3. Transition of care communication with outpatient health professionals |
All 665 Aged> 70 IG = 317 CG = 348 |
ED visit | 3 months after D/C 6 months after D/C |
N = 317 n = 11 3.8% n = 19 6.0% |
N = 348 n = 12 3.4% n = 22 6.3% |
NR |
| Mi et al. (2018) | Rochester, NY and Madison, USA | Single-blinded RCT |
Postdischarge: 1. Home visit 2. Phone call visit |
2400 patients over the age of 60 were enrolled. | ED visit | 1 month after D/C | NR | NR | NR |
| Occelli et al. (2016) | The Rhône-Alpes region of France | A stepped-wedge cluster randomized experiment using a multicentre-design |
Predischarge: 1. Discharge care plan Postdischarge: 1. Follow-ups |
630 patients aged> 75 | ED visit | 30 days after D/C | NR | NR | NR |
| Wee et al. (2014) | Five hospitals in Singapore | A retrospective cohort study |
Predischarge: 1. Coaching 2. Care plan Postdischarge: 1.Follow-ups |
IG = 4132 CG = 4132 aged >65 |
Hospitalization; ED visits |
1 month after D/C 6 months after D/C |
N = 4132 n = 992 19.3% n = 3801 46.3% |
N = 4132 n = 1240 32% n = 4545 57.9% |
OR = 0.81(0.72-0.90) p <.001 0.90 (0.82-0.99) p =.03 |
IG= intervention group, CG= control group
Predischarge: Transitional care interventions that are implemented before discharge
Postdischarge: Transitional care interventions are those that are undertaken after a patient is discharged
Transitional care intervention: Interventions assist elderly persons in regaining their independence following a hospital stay. It is provided either before or after the discharge of older patients
ED visit: The ED visits after discharge from hospital/ED in measured time (1,2,3,6 and 12 months after discharge)
The effect of the intervention on the outcome: reduced ED visit
NR = not report
Study Population
This review included roughly 16,105 patients, with 6750 in the intervention groups and 9,355 in the control groups. The participants in the intervention groups were on average 82 years old (range 77.7–85.9), while those in the control groups were on average 82 years old (range 77.9–86.4).
Transitional Care Interventions (TCIs)
The strength of each TCI is described in Table 4. Verhaegh et al. (2014) came up with the idea of calculating intervention intensity. Only one study was classified as low intensity (Sabir et al., 2019)). The majority of included studies have a high intensity (Enguidanos et al., 2012; Heeren et al., 2019; Kim et al., 2021; Lee et al., 2018; Legrain et al., 2011; Liang et al., 2021; Low et al., 2015; Mi et al., 2018; Occelli et al., 2016; Robinson et al., 2021; Schapira et al., 2021; Wee et al., 2014). The vast majority of high-intensity interventions had a beneficial influence on ED visits, but one low-intensity intervention also had a good impact. The effects of high-intensity interventions were bigger and statistically significant.
| Author | Assessment at admission | Self-management education | Caregiver involvement | Discharge planning | Care coordination by the nurse | Primary care provider communication | Home visit within three days | Number of the home visit | Telephone follow-up | Number of telephone follow-up | The total duration of intervention | The total score of intervention intensity |
|---|---|---|---|---|---|---|---|---|---|---|---|---|
| Schapira et al. (2021) | / | / | / | / | / | / | / | 3 | 10 | |||
| Robinson et al. (2021) | / | / | / | / | / | / | 1 | 1 | 3 | 11 | ||
| Low et al. (2015) | / | / | / | / | / | / | / | 1 | 3 | 11 | ||
| Heeren et al. (2019) | / | / | / | / | / | 1 | 2 | 3 | 11 | |||
| Lee et al. (2018) | / | / | / | / | / | / | / | 1 | 3 | 11 | ||
| Sabir et al. (2019) | / | / | 3 | 5 | ||||||||
| Liang et al. (2021) | / | / | / | / | / | 1 | 3 | 9 | ||||
| Kim et al. (2021) | / | / | / | / | 1 | 2 | 3 | 10 | ||||
| Enguidanos et al. (2012) | / | / | / | / | / | / | / | 3 | 1 | 2 | 3 | 16 |
| Legrain et al. (2011) | / | / | / | / | / | / | 3 | 9 | ||||
| Mi et al. (2018) | / | / | / | / | 1 | 1 | 2 | 1 | 9 | |||
| Occelli et al. (2016) | / | / | / | / | / | 2 | 1 | 2 | 1 | 11 | ||
| Wee et al. (2014) | / | / | / | / | 2 | 1 | 2 | 3 | 12 |
Note: / symbol for yes
The ED visits in these studies were monitored over a period ranging from one month to twelve months after hospital discharge. Eight studies looked at ED visits six months after discharge (Enguidanos et al., 2012; Kim et al., 2021; Lee et al., 2018; Legrain et al., 2011; Liang et al., 2021; Low et al., 2015; Sabir et al., 2019; Schapira et al., 2021), and seven studies looked at three months after discharge (Heeren et al., 2019; Kim et al., 2021; Lee et al., 2018; Legrain et al., 2011; Liang et al., 2021; Low et al., 2015; Wee et al., 2014), five studies observed at one month after discharge (Heeren et al., 2019; Kim et al., 2021; Mi et al., 2018; Occelli et al., 2016; Wee et al., 2014). The rest (just one trial) was assessed either two months after discharge (Kim et al., 2021) or one year after discharge (Robinson et al., 2021). At one month, two months, and three months after discharge, a high-intensity TCI intervention would considerably reduce ED visits for older adults. However, the results on the intensity of the intervention are ambiguous six months after discharge because two studies with high-intensity treatments found no significant differences between the two groups in any of the ED visits (Lee et al., 2018; Legrain et al., 2011), while one study with a low-intensity intervention found a beneficial effect on ED visits (Sabir et al., 2019). Furthermore, 12-month high-intensity intervention has a beneficial influence on ED visits, according to one study (Robinson et al., 2021).
Predischarge Components (TCIs before discharge from hospital)
A comprehensive geriatric assessment, tailored recommendations to minimize geriatric syndromes, planned transition of care, care plan, self-management education, a patient information leaflet, and a web page, wireless transmission devices, medication counseling, comprehensive chronic medication review, transition-of-care communication with outpatient health professionals, discharge care planning, and coaching were all included in predischarge components across studies. The most widely used TCIs of predischarge intervention in these articles that were helpful in reducing ED visits among older persons were care planning, the transition of care, and self-management education.
Post Discharge Components (TCIs after discharge from hospital)
A health and social care counselor, regular follow-up, a comprehensive needs assessment, an individualized care plan, rehabilitation, cognitive and memory training, information/outcome referral to community pharmacist, telemonitoring through wireless transmission devices, home visit, phone visit, face-to-face demonstration, and health education were all included in the postdischarge components. Follow-ups, home visits, and phone calls were the most commonly employed TCIs of postdischarge intervention in these papers that were helpful in reducing ED visits among older persons.
Risk of Bias in Included Studies
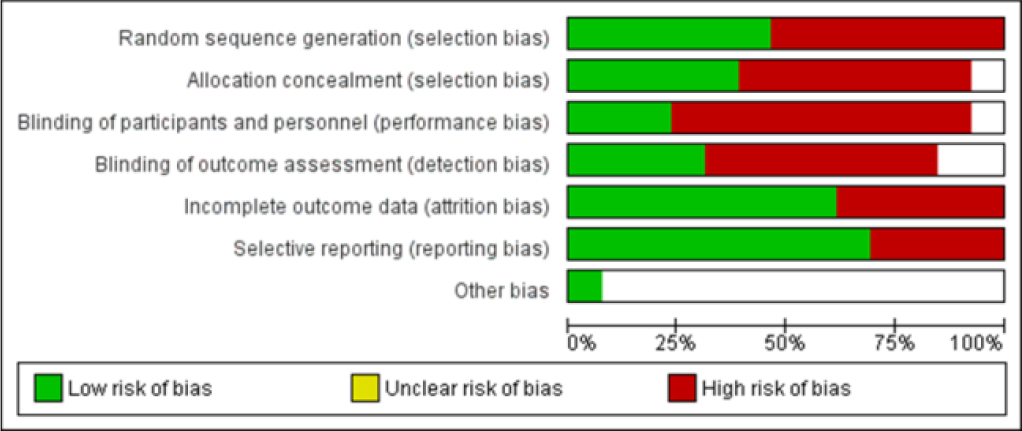
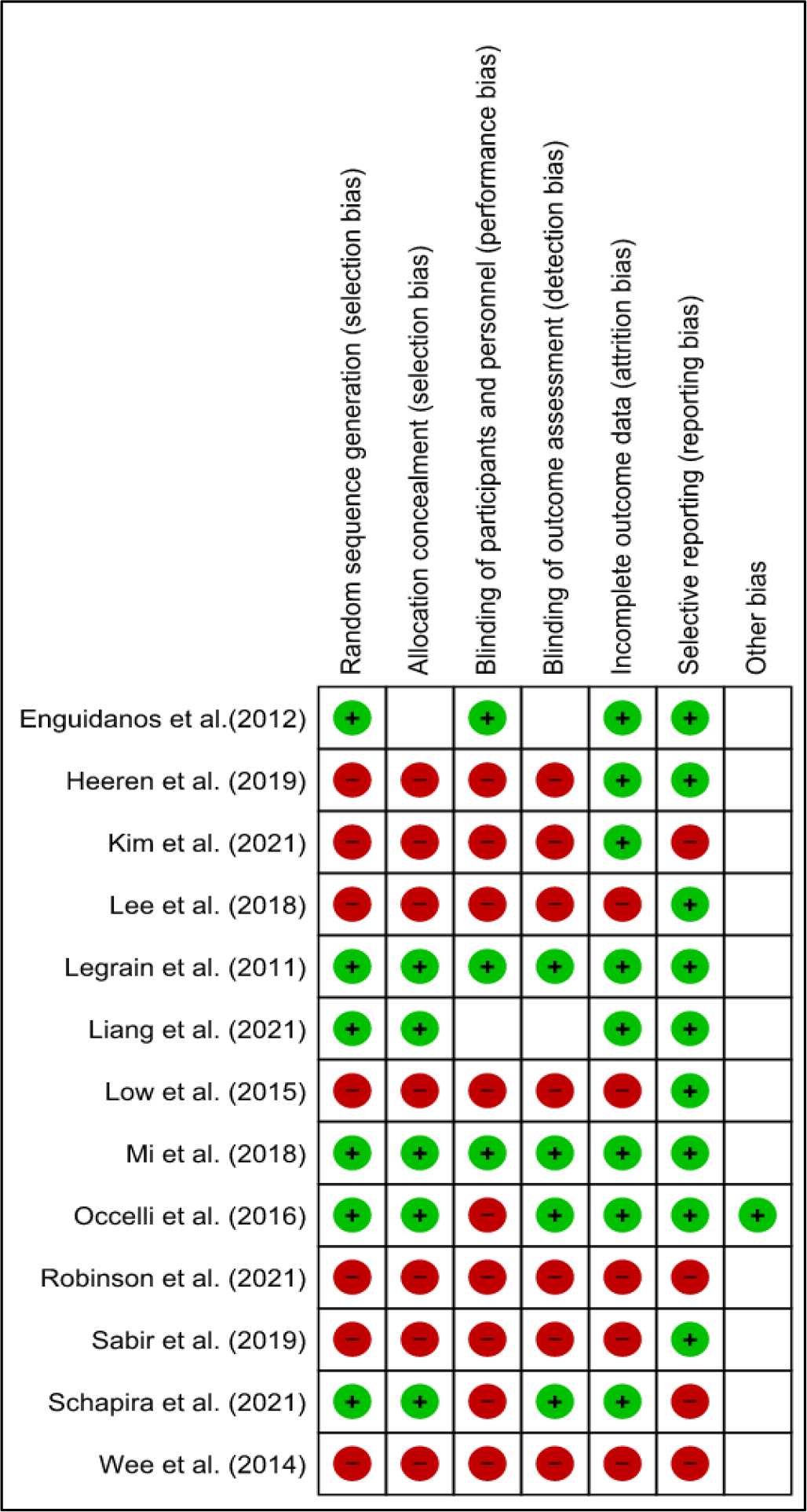
Figure 2 and Figure 3 show the overall judgment scores for each risk of bias item. Ten of the thirteen trials (76.9%) showed a high risk of bias owing to insufficient randomization, allocation concealment, and blinding (Enguidanos et al., 2012; Heeren et al., 2019; Kim et al., 2021; Lee et al., 2018; Liang et al., 2021; Low et al., 2015; Robinson et al., 2021; Sabir et al., 2019; Schapira et al., 2021; Wee et al., 2014). There was a moderate probability of bias in three studies (23.1%) (Legrain et al., 2011; Mi et al., 2018; Occelli et al., 2016). The overall risk of bias was considerable in the majority of the included trials due to different shortcomings in the randomization procedure in older persons. Older persons are commonly underrepresented in RCTs (Broekhuizen et al., 2015). As a result, clinical trial participants rarely represent older patients in general medical practice, putting RCTs’ external validity in the older patient population in jeopardy (Kennedy-Martin et al., 2015). In addition, evidence-based treatment has limited application in this population because older people are usually excluded from clinical trials (Fougère et al., 2016). As a result, the scope of the RCT investigation among these people is limited. Therefore, investigations with a high chance of bias are still required.
Synthesis of Results
When it came to the impact on the outcome, all studies (100%) showed a positive impact on ED visits 1, 2, and 3 months following hospital discharge, but not on TCIs conducted after six months (Lee et al., 2018; Legrain et al., 2011). Only three of the thirteen research studies (Liang et al., 2021; Robinson et al., 2021; Wee et al., 2014) provided an impact size estimate. Odds ratios (ORs) ranged from -0.07 to 0.90. One study provides an impact size by using a Risk Ratio (RR) (Schapira et al., 2021) ranging from 0.562 to 0.929. Because only four of the 13 studies provided the risk ratio and odds ratios, it was unable to calculate RRs and ORs and their 95 percent confidence intervals for those studies.
Meta-Analysis
Because most of the included studies had a significant risk of bias and differences in follow-up measurement intervals and multi-component characteristics, only three studies mentioned odd ratios, and meta-analytic pooling for impact estimations of effect size was problematic.
Discussion
According to our data, the majority of interventions in the transitional period between hospital and home appeared to reduce the rate of ED visits among older patients discharged from the ED and a medical ward. TCIs undertaken more than six months after discharge from the hospital, on the other hand, gave inconclusive results. There are several possible causes for these inconsistencies, as discussed below.
Our findings indicate that the intensity of interventions has an impact on the rate of ED visits. High-intensity interventions had a greater impact than low-intensity interventions in general. This is consistent with prior findings (Verhaegh et al., 2014), which show that intervention components that appear to be the same across trials might have different characteristics. The varied influence on ED visits could be due to differences in intervention components between trials. A cross-study intervention component analysis to establish which components have a positive influence on ED visits is impossible. A full geriatric assessment, need assessment, discharge planning, caregiver involvement, self-management education, coaching, home visits, and telephone call visits were all components of interventions that had a positive influence on ED visits. Furthermore, the timing of the outcome evaluation influences the chance of a preventive ED visit. The findings of this study imply that interventions with high intensity and duration at 1, 2, and 3 months after discharge from the hospital are beneficial.
Several of the studies included did not account for potential confounders such as growing age, gender, psychological problems, poor general health (Sheikh, 2019), previous experience history, living in a rural location, low income, polypharmacy, comorbidity, and dementia (Dufour et al., 2019). Internal validity and the influence on ED visit rates may have been harmed as a result of these factors. Furthermore, randomized controlled trials (RCTs) made up less than half of the research considered (Enguidanos et al., 2012; Legrain et al., 2011; Liang et al., 2021; Mi et al., 2018; Occelli et al., 2016; Schapira et al., 2021). As a result, ED visit rates in these studies may be skewed.
The bulk of the included studies had poor methodological quality, indicating a substantial risk of bias. A low measure grade can show poor methodological quality and inadequate reporting techniques. The latter makes determining the genuine quality and the possibility of bias challenging. If the low ranking is due to insufficient methodological reporting, the effects may be unaffected. If the poor rating is due to methodological issues, however, it is likely to underestimate the true impact of the interventions. The research design and confounders component receive the lowest score. Because older adults are frequently omitted from clinical trials, RCTs and consideration of confounder variables are not always possible in older adult population research (Fougère et al., 2016). Furthermore, no matter how many variables the researcher controls for, residual confounding will exist, maybe due to unknown and unmeasured causes (Skelly et al., 2012). As a result, the low rating of methodological quality in study design and managing confounder variables is thought to be linked to the numerous constraints of doing research with the elderly.
Study Limitation
This review tries to synthesize the existing transitional care program between hospital and home, with the goal of reducing postdischarge ED visits for older patients. Although the analysis highlights the benefits of transitional care interventions in improving ED visits in these populations, it also identifies some potential limits. Small studies were considered; searches were limited to English-language literature, and studies in this population were few. We also didn’t have enough research to do a meta-analysis because only four studies examined the transitional care intervention’s effect size. As a result, the most effective transitional care treatments for reducing ED in this population are unclear.
Implications of this Study for Nursing Practice
In terms of clinical implications, nurses should plan for a high-intensity transitional care intervention that includes both pre-and postdischarge interventions in order to reduce ED visits by older patients. Future meta-analyses will be required to determine the efficacy of transitional care interventions.
Conclusion
The majority of TCIs have a beneficial influence on ED visit rates among older patients, with the greatest benefit occurring less than six months following discharge. As a result, we feel that the present evidence supports the recommendation of pre-discharge and postdischarge transitional care. However, there is insufficient data to propose a specific intervention. The major finding is that high-intensity therapies had a pronounced favorable impact within less than six months of discharge. However, this should be seen in the context of the fact that only 13 research matched the inclusion criteria, and the methodological quality approach assigned a low level of certainty to the evidence.