









Background
Childbirth is a physiological process that involves a sequential, gradual, and integrated set of changes within the birth canal to end with the delivery of the fetus and the placenta (Modoor et al., 2021; Ricci, 2012). Putting laboring women in a relaxed position is vital to help them to deal well with these changes, reduce pain and facilitate normal delivery (White et al., 2011). Moreover, maternal positioning during childbirth affects childbirth progress. At the same time, it can reduce the need for the induction or augmentation of delivery and manage pain and stress (Watson & Cooke, 2018).
Positions for women in childbirth can be categorized into upright positions as standing, sitting, kneeling, squatting, walking, and on all fours, and recumbent positions as lateral, supine, and semi-recumbent (Kemp et al., 2013). In the upright position, gravity reduces aortocaval compression, which makes the uterine contractions more effective and ensures better fetal alignment in the birth canal (Gizzo et al., 2014). In this context, the results from an experimental study demonstrated that adopting an upright position in the first stage of childbirth, when the cervix was dilated 2–4 cm, reduced pain, improved the effectiveness of uterine contractions, decreased the rate of cesarean birth, perineal trauma, an episiotomy, and significantly decreased the use of analgesics (Deliktas & Kukulu, 2018). Furthermore, Emam and Al-Zahrani (2018) reported that using the upright position positively impacted the progress of childbirth by increasing the effectiveness of the uterine contractions and facilitating cervical dilatation and fetal descent, compared to the recumbent position, and this finding had statistical significance. In contrast, the adoption of the upright position throughout childbirth was not shown to have a statistically significant impact on the duration and mode of delivery (Deliktas & Kukulu, 2018).
Elsewhere, the recumbent position may be used by women during childbirth because of being recommended at admission (Mselle & Eustace, 2020). Using a recumbent position during birth may be seen as beneficial by some healthcare providers to palpate the maternal abdomen, assess uterine contractions, presentation, and position, listen to the fetal heart rate (FHR), and conduct vaginal exams efficiently. However, it can inhibit the progress of childbirth as the gravid uterus compresses the abdominal blood vessels and impairs circulation, including uteroplacental perfusion, which may adversely affect maternal and fetal well-being (Cunningham et al., 2009).
More and more people worldwide are paying attention to the standard of maternity care. Further, it is evaluated against using updated and evidence-based hospital guidelines for birth management (Altaweli et al., 2014). The selection of a maternal birth position is a vital aspect of midwifery care during childbirth; however, in many cases, it may be neglected by some healthcare providers. Adopting a recumbent position in delivery is a common practice in the current century, although it should only be adopted when indicated (Desseauve et al., 2017).
There is a lack of consensus on the impacts of different maternal positions during childbirth on maternal, fetal, and neonatal outcomes. Available evidence in this field is controversial and fragmented. In addition, a scarce of studies have assessed the effects of the upright and recumbent positions on childbirth outcomes during the first stage of childbirth, especially in the Kingdom of Saudi Arabia (Emam & Al-Zahrani, 2018). Thus, it is essential to identify other maternal birth positions that could be used during childbirth’s first stage and understand how they impact childbirth outcomes.
Women giving birth must comprehend the advantages and disadvantages of each position and be encouraged to choose a position that will provide them with the most incredible comfort, control, and benefits (Lawrence et al., 2013). In this regard, midwives play an important role in collaborating with other healthcare professionals regarding providing adequate care to women in childbirth. To help laboring women make informed decisions regarding their positions, nurses or midwives must provide concise, consistent, and evidence-based descriptions of the hazards and advantages of each position (Cunningham et al., 2009; Oats & Abraham, 2017). In addition, nurses and midwives should consider each pregnant woman’s feelings and identify the obstetric factors that may interfere with the chosen birthing position (Priddis et al., 2012). One of the critical areas of practice is the mother’s position during the early labor stage. Despite an increasing body of evidence demonstrating the physical advantages for women and fetuses when they use an upright posture during childbirth, the majority of women around the globe give birth to their children while laying on their backs in bed, with a few notable exceptions, a practice that is not supported by empirical evidence.
In the past, the use of the supine position was encouraged by traditional and former practitioners. Since then, the benefits of the upright position have been revealed, and research backs them up; this position has subsequently been encouraged by some midwives and obstetricians, and it is requested by women in childbirth (Gizzo et al., 2014). Unfortunately, the impact of upright versus recumbent postures during the first stage of birth on the mother, fetus, and newborn is rarely agreed upon, and the evidence in this field is frequently disputed and fragmentary.
The World Health Organization (WHO) ended with no evidence to back up using a recumbent posture in early labor. However, it is shown that upright positions during early labor reduce the need for interference and the duration of childbirth while having little impact on the well-being of the mother and fetus. Consequently, midwives and nurses should allow women to assume whichever position is most comfortable for them during the first stage of childbirth (World Health Organization, 2018).
Considering that few studies had addressed the impact of different postures on childbirth outcomes in Saudi Arabia, the current research aimed to evaluate the effect of the upright compared to the recumbent postures on birth outcomes in Jeddah. There are four hypotheses for this study; it was assumed that women who adopted the upright position during first-stage childbirth would experience (1) faster progress with their childbirth, (2) shorter childbirth duration, (3) less pain, and (4) more satisfaction with this position than women who used the recumbent posture.
Methods
Study Design
The study used a quasi-experimental design.
Participants/Samples
The setting for this study was the childbirth unit at East Jeddah Hospital, under the auspices of the Ministry of Health of KSA.
The inclusion criteria of the sample were women in the active phase of first-stage childbirth, aged 18–45 years, with normal body mass index, pregnant with a single fetus with the cephalic presentation, term pregnancy (38–41 weeks), and had the willingness to be part of the study. While high-risk pregnant women (Gestational diabetic Mellitus, cardiac disease, pre-eclampsia placenta previa & abruption placenta), elective cesarean section, malposition, induced or augmented childbirth, meconium-stained amniotic fluid, and epidural anesthesia were excluded.
The sample size was estimated to be 300 using an online Raosoft® sample calculator (http://www.raosoft.com). The input data were a population size of 1,267 over six months (Ministry of Health of Saudi Arabia, 2019), 5.0% acceptable error of margin, 95% level of confidence, and 50% response rate.
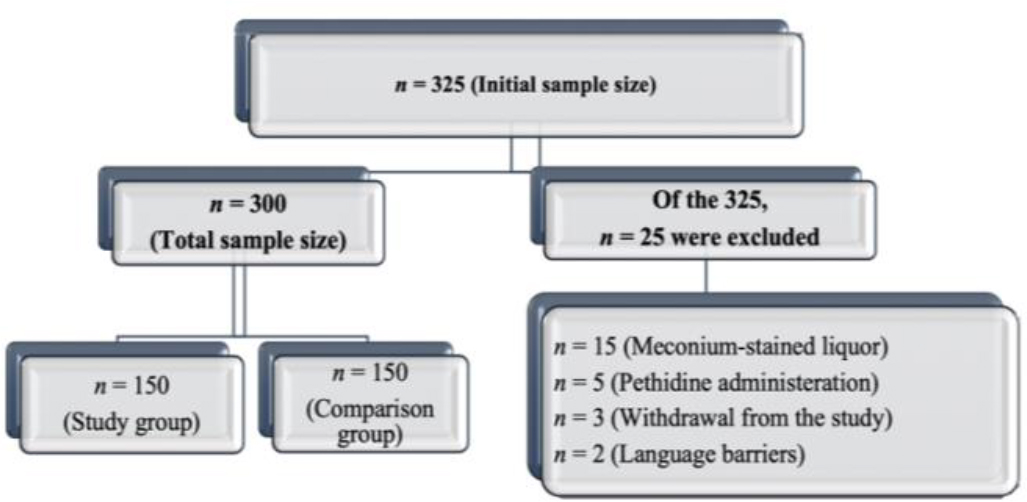
Purposive sampling was used to recruit 300 eligible laboring women. Afterward, the participants were categorized into two groups, 150 each: upright position (Study group) and recumbent position as routinely used for maternity care in the study setting (Comparison group). Twenty-five women were excluded after recruitment owing to the presence of meconium-stained amniotic fluid, the administration of pethidine, withdrawal from the study, or language barriers (Figure 1).
Instruments
A structured questionnaire: the modified WHO partograph and the Wong-Baker FACES® Pain Rating Scale were used to obtain the needed data. The first part of the questionnaire elicited information on the sociodemographic background of the participants, such as age, residence, occupation, educational level, gestational age, gravidity, and parity.
The second part assessed maternal satisfaction with the adopted position. If a mother would use it in the subsequent childbirth through two questions, their answers were evaluated by a 5-points Likert scale from 0–4 (Emam & Al-Zahrani, 2018). Permission to use this part was obtained from the corresponding author by email.
The Modified World Health Organization partograph was used to graphically determine childbirth progress using data pertaining to dilatation of the cervix, fetal descent, and contractions of the uterus (frequency, duration & intensity), the duration of the first, second, and third stages of childbirth and the method of delivery (World Health Organization, 2018).
The Wong-Baker FACES Foundation (2019) was used after the researchers explained the scoring system to the participants. Then, they were requested to select the best face that depicted the experienced pain.
The validity of the data collection tools was ensured by a review of experts in the field of obstetrics and gynecology who assessed their relevancy and appropriateness to meet the study’s aim. Reliability was evaluated by pilot testing of the instruments to ensure their consistency. A pilot study was conducted by pre-testing the tools on 10% of the sample (30 women in childbirth) eligible for the study to assess their applicability, consistency, and accuracy and to determine the needed time to complete the research and potential challenges that may hinder the data collection (Polit & Beck, 2018).
The pilot study data were reviewed and subjected to statistical analysis. The total reliability of the data measurement scale was 0.63.
Data Collection
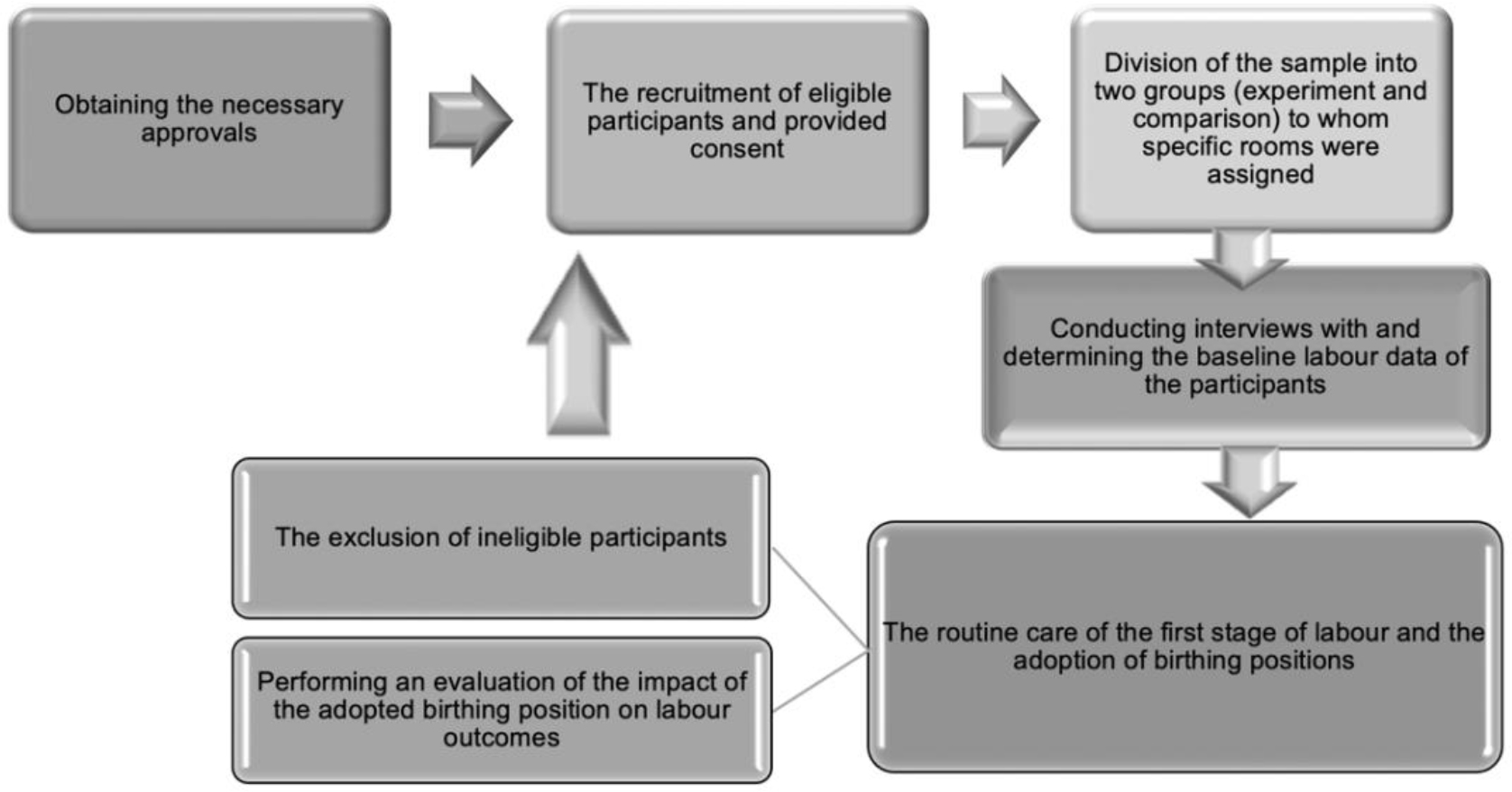
Data collection was completed in five months (November 2020-March 2021). Data collection started by explaining the aim and objectives of the study to nurses/midwives in the childbirth unit at East Jeddah Hospital. Then, the researchers selected two rooms for the comparison group and two for the experiment group. Next, data were collected through interviews, assessments, implementation, and evaluation phases (Figure 2).
Interview phase. The researcher explained the aim and study details to women before obtaining their consent. After that, the participants were interviewed to collect sociodemographic data.
Assessment phase. The standard data on childbirth progress, such as contractions of the uterus (frequency, duration & strength), dilatation of the cervix, fetal descent, and pain levels, were collected upon the admission of the participants to the unit.
Implementation phase. While in childbirth, the participants in both groups received intravenous fluids, back massage, and prescribed paracetamol. In addition to testing for COVID-19 as routine care in the first stage of childbirth, according to the hospital policy. The researchers explained the different types of an upright position and their benefits to each woman in the study group; then, the participant was requested to adopt an upright position of choice for 15–20 minutes each hour and return to bed in between for 10–15 minutes. The selected positions included sitting on a birthing ball with support, on all fours, and squatting. Participants in the comparison group adopted either a supine or lateral position.
Evaluation phase. The researchers evaluated the effects of the upright and recumbent positions on childbirth progress hourly using the data collection tools in terms of the interval, frequency, and duration of contractions of the uterus, dilatation of the cervix, and fetal descent, as well as pain levels and maternal satisfaction with the adopted position.
Data Analysis
The Statistical Package managed data for Social Sciences®, version 25 for Windows®. Frequencies, percentages, means, and standard deviations were used for data presentation. Chi-square, independent t-test, and paired t-test were also used to assess the association and significance of the finding between the study variables and to test the study hypotheses. A significant difference was set at ≤0.05.
Ethical Considerations
The research was performed after being reviewed and approved by the Research Unit in the College of Nursing, the King Abdullah International Medical Research Center, and the institutional review board (IRB) at King Abdulaziz Medical City, Western Region, Jeddah, KSA. Approval from the IRB of the Ministry of Health, KSA, was also granted, and the administrative personnel in East Jeddah Hospital were contacted before beginning data collection. The researcher clarified the study’s aim and nature to women who met the criteria for inclusion and obtained their informed consent for participation. It was clear to the women that their involvement in the study was voluntary, and they had the right to revoke it at any moment. Privacy and anonymity were kept.
Results
The mean age of the participants in the experiment group was 32.20 ± 28.37 years, with 43.3% of them aged 26 to 30 years as compared to 30.50 ± 5.3 years, with 40.0% of them aged 31 to 35 years in the comparison group. In addition, in the experiment group, 74.7% received university or higher education, 62% were housewives, 54.7% were living in urban areas, and 92.7% were Saudi, compared to 62.7%, 55.3%, 44.7%, and 90.7%, respectively in the comparison group. Finally, the mean gestational age during delivery was 39.1 ± 2.93 weeks in the experiment group compared to 39.2 ± 3.99 weeks in the comparison group which reflected no statistically significant differences between the two groups (Table 1).
| Variable | Upright position (experiment group) | Recumbent position (comparison group) | ||
|---|---|---|---|---|
| n | % | n | % | |
| Age in years | ||||
| 20 to 25 | 31 | 20.7 | 39 | 26.0 |
| 26 to 30 | 65 | 43.3 | 28 | 18.7 |
| 31 to 35 | 43 | 28.7 | 60 | 40.0 |
| ≥35 | 11 | 7.3 | 23 | 15.3 |
| Mean ± SD | 32.20 ± 28.37 | 30.50 ± 5.3 | ||
| x2= 377.43 p = 0.49 | ||||
| Educational level | ||||
| Secondary | 38 | 25.3 | 56 | 37.3 |
| University or higher | 112 | 74.7 | 94 | 62.7 |
| x2= 1.19 p = 0.27 | ||||
| Occupation | ||||
| Work-related to the health sector | 14 | 9.3 | 9 | 6.0 |
| Work not related to the health sector | 43 | 28.7 | 58 | 38.7 |
| Housewife | 93 | 62.0 | 83 | 55.3 |
| x2= 3.09 p = 0.54 | ||||
| Residence | ||||
| Rural | 68 | 45.3 | 83 | 55.3 |
| Urban | 82 | 54.7 | 67 | 44.7 |
| x2= 1.04 p = 0.23 | ||||
| Nationality | ||||
| Saudi | 139 | 92.7 | 136 | 90.7 |
| Non-Saudi | 11 | 7.3 | 14 | 9.3 |
| x2= 0.001 p = 0.97 | ||||
| Gestational age in weeks | ||||
| Mean ± SD | 39.1 ± 2.93 | 39.1 ± 2.93 | ||
| x2= 544.11 p = 0.94 | ||||
The mean baseline duration of uterine contractions in seconds among the participants in the experiment group was 36.76 ± 7.9 compared to 38.76 ± 10.63 in the comparison group and reflected no statistically significant difference (p < 0.06).
After the interventions, the mean duration of uterine contractions was higher among participants in the experimental group than among the participants in the recumbent position, reflecting a statistically significant difference in childbirth outcomes between the two groups, particularly after two hours (t298 = 92.10, p = 0.001), three hours (t248 = 240.83, p = 0.001), and four hours (t12 = 2.11, p = 0.04).
In addition, the intervals between uterine contractions reflect a statistically significant difference after two hours (t298= 2.68, p = 0.001), three hours (t248 = 2.23, p = 0.03), and four hours (t280 = 12, p = 0.02), respectively. Also, there was a statistically significant difference in the number of uterine contractions per 10 minutes, especially after one hour (t298 = 3.07, p = 0.001), two hours (t298= 3.69, p = 0.001), and three hours (t248= 4.12, p = 0.001), but not after four hours (t12= 1.55, p = 0.16) (Table 2).
| Variable | Upright position (experiment) | Recumbent position (Comparison) | Independent t-test | df | p-value | ||
|---|---|---|---|---|---|---|---|
| n | Mean ± SD | n | Mean ± SD | ||||
| Duration of uterine contractions in seconds | |||||||
| Baseline | 150 | 36.76 ± 7.9 | 150 | 38.76 ± 10.63 | 1.83 | 298 | 0.07 |
| After one hour | 150 | 44.46 ± 9.8 | 150 | 42.00 ± 12.28 | 1.84 | 298 | 0.67 |
| After two hours | 150 | 58.00 ± 6.02 | 150 | 51.80 ± 11.81 | 92.10 | 298 | 0.001* |
| After three hours | 125 | 60.00 ± 0.00 | 125 | 57.69 ± 5.77 | 240.83 | 248 | 0.001* |
| After four hours | 7 | 60.00 ± 5.90 | 7 | 60.89 ± 5.99 | 2.11 | 12 | 0.04* |
| Intervals between uterine contractions in minutes | |||||||
| Baseline | 150 | 3.50 ± 0.63 | 150 | 3.54 ± 0.63 | 0.56 | 298 | 0.57 |
| After one hour | 150 | 3.18 ± 0.50 | 150 | 3.28 ± 0.50 | 1.77 | 298 | 0.07 |
| After two hours | 150 | 2.97 ± 0.25 | 150 | 3.09 ± 0.49 | 2.68 | 298 | 0.001* |
| After three hours | 125 | 2.76 ± 0.33 | 125 | 2.86 ± 0.34 | 2.23 | 248 | 0.03* |
| After four hours | 7 | 2.5 ± 0.04 | 7 | 2.85 ± 0.23 | 2.80 | 12 | 0.02* |
| Number of uterine contractions per 10 minutes | |||||||
| Baseline | 150 | 2.60 ± 0.49 | 150 | 2.56 ± 0.49 | 1.08 | 298 | 0.278 |
| After one hour | 150 | 2.92 ± 0.54 | 150 | 2.74 ± 0.436 | 3.07 | 298 | 0.001* |
| After two hours | 150 | 3.18 ± 0.39 | 150 | 3.01 ± 0.46 | 3.69 | 298 | 0.001* |
| After three hours | 125 | 3.56 ± 0.49 | 125 | 3.28 ± 0.53 | 4.12 | 248 | 0.001* |
| After four hours | 7 | 3.14 ± 0.37 | 7 | 3.29 ± 0.46 | 1.55 | 12 | 0.16 |
In addition, Table 3 shows that there was a significant difference in the intensity of uterine contraction between the experimental and control groups, especially after two hours (X2 = 5.03, p = 0.02) and three hours (X2 = 23.08, p = 0.001).
| The intensity of uterine contraction | Upright position (experiment) | Recumbent position (comparison) | Test of significant | p-value | |||
|---|---|---|---|---|---|---|---|
| n | % | n | % | ||||
| Baseline | Mild | 6 | 4.0 | 1 | 0.7 | X2 = 1.99 | 0.13 |
| Moderate | 115 | 76.7 | 115 | 76.7 | |||
| Severe | 29 | 19.3 | 34 | 22.7 | |||
| After 1 hour | Moderate | 88 | 58.7 | 73 | 48.7 | X2 = 3.01 | 0.08 |
| Severe | 62 | 41.3 | 77 | 51.3 | |||
| After 2 hours | Moderate | 16 | 10.7 | 30 | 20.0 | X2 = 5.03 | 0.02* |
| Severe | 134 | 89.3 | 120 | 80.0 | |||
| After 3 hours | Moderate | 1 | 0.7 | 2 | 1.3 | X2 = 23.08 | 0.001* |
| Severe | 124 | 99.3 | 123 | 82.0 | |||
| After 4 hours | Moderate | 0 | 0 | 1 | 16.66 | X2 = 0.74 | 0.38 |
| Severe | 7 | 100 | 6 | 83.34 | |||
Table 4 shows that there was greater progress in cervical dilatation after three hours among the participants in the upright position group than among those in the recumbent position group, with a highly statistically significant difference between the two groups (t248 = 2.6, p <0.001). Similarly, there was progress of foetal descent was greater among the participants in the upright position group than among those in the recumbent position group, with a high statistically significant difference especially after one hour (t298 = 7.04, p <0.001), two hours (t298 = 9.55, p <0.001), three hours (t248 = 13.97, p < 0.001), and four hours (t12 = 0.00, p <0.02), respectively. In addition, there was a significant difference in pain scores between the two groups after one hour (t298 = 18.52, p <0.001), two hours (t298 = 90.81, p < 0.001), and three hours (t248 = 109.38, p <0.001), respectively (Table 4).
| Variable | Upright position (experiment) | Recumbent position (comparison) | Independent t-test | df | p-value | ||
|---|---|---|---|---|---|---|---|
| n | Mean ± SD | n | Mean ± SD | ||||
| Cervical dilatation (cm) | |||||||
| Baseline | 150 | 5.31 ± 0.80 | 150 | 5.30 ± 0.85 | 0.73 | 298 | 0.44 |
| After one hour | 150 | 6.28 ± 0.58 | 150 | 6.36 ± 0.92 | 1.01 | 298 | 0.32 |
| After two hours | 150 | 7.9 ± 0.72 | 150 | 7.84 ± 1.11 | 0.57 | 298 | 0.54 |
| After three hours | 125 | 9.6 ± 0.69 | 125 | 9.36 ± 1.02 | 2.6 | 248 | 0.001* |
| After four hours | 7 | 10 ± 0.00 | 7 | 9.53 ± 0.71 | 1.01 | 12 | 0.34 |
| Fetal head descent/fifths | |||||||
| Baseline | 150 | -2.52 ± 0.69 | 150 | -2.42 ± 0.61 | 1.18 | 298 | 0.22 |
| After one hour | 150 | -1.66 ± 0.68 | 150 | -2.21 ± 0.71 | 7.04 | 298 | 0.001* |
| After two hours | 150 | -0.35 ± 0.60 | 150 | -1.21 ± 0.92 | 9.55 | 298 | 0.001 * |
| After three hours | 125 | 1.18 ± 0.87 | 125 | 0.32 ± 0.81 | 13.97 | 248 | 0.001 * |
| After four hours | 7 | 0.33 ± 0.57 | 7 | 0.33 ± 0.57 | 0.00 | 12 | 0.02 * |
| Mean pain scores | |||||||
| Baseline | 150 | 3.05 ± 1.00 | 150 | 3.09 ± 0.99 | 0.55 | 298 | 0.55 |
| After one hour | 150 | 5.02 ± 1.04 | 150 | 6.69 ± 1.11 | 18.52 | 298 | 0.001* |
| After two hours | 150 | 6.7 ± 1.13 | 150 | 8.61 ± 1.08 | 90.81 | 298 | 0.001 * |
| After three hours | 125 | 8.13 ± 1.24 | 125 | 9.08 ± 1.00 | 109.38 | 248 | 0.001* |
| After four hours | 7 | 8.38 ± 1.24 | 7 | 9.00 ± 1.00 | 108.99 | 12 | 0.51 |
Table 5 shows that the duration of the first stage was under 5-6 hours for 74.64% of the experiment group compared to 61.34% of the comparison group. Only 0.66% of the experiment group had >7 hours in the first stage of childbirth compared to 24.66% of the comparison group. The mean duration of the first stage of birth in hours among participants in the experiment and comparison groups was 5.88 ± 0.29 and 6.27 ± 0.68, respectively, with a highly statistically significant difference at (t202 = 6.22, p = 0.001). The second stage of childbirth duration was <30 minutes for 80% of participants in the experiment group compared to 76% in the comparison group. There was a statistically significant difference between the two groups regarding the duration of the second stage of childbirth (t232 = 3.44, p = 0.001) and the third stage of birth (t272 = 14.92, p = 0.001).
| Variable | Upright position | Recumbent position | Independent t-test | df | p-value | ||
|---|---|---|---|---|---|---|---|
| n | % | n | % | ||||
| Duration of the first stage of childbirth in hours | |||||||
| 5-6 | 112 | 74.6 | 92 | 61.3 | 6.22 | 202 | 0.001 ** |
| 6-7 | 37 | 24.7 | 21 | 14.00 | 56 | ||
| >7 | 1 | 0.6 | 37 | 24.6 | 36 | ||
| Mean ± SD | 5.88 ± 0.29 | 6.27 ± 0.68 | |||||
| Duration of the second stage of childbirth in minutes | |||||||
| <30 | 120 | 80.0 | 114 | 76.0 | 3.44 | 232 | 0.001** |
| 30-60 | 30 | 20.0 | 33 | 22.0 | 61 | ||
| >60 | 0 | 0.0 | 3 | 2.0 | 1 | ||
| Mean ± SD | 25.3 ± 9.11 | 29.30 ± 1033 | |||||
| Duration of the third stage of childbirth in minutes | |||||||
| 10-20 | 145 | 96.7 | 129 | 86.0 | 14.92 | 272 | 0.001 ** |
| 20-30 | 5 | 3.3 | 21 | 14.0 | 24 | ||
| Mean ± SD | 10.33 ± 1.80 | 15.83 ± 4.07 | |||||
Table 6 shows statistically significant differences between the two groups with the type of membrane rupture (X2 = 27.4, p = 0.001). Of the participants in the experiment group, 57.3% had normal vaginal delivery compared to 44.70% of participants in the comparison group, with a highly statistically significant difference at (X2= 7.42, p = 0.001).
| Variable | Upright position | Recumbent position | Test of significant | p-value | ||
|---|---|---|---|---|---|---|
| n | % | n | % | |||
| Type of membranes rupture | ||||||
| AROM | 79 | 52.7 | 72 | 48.0 | X2 = 27.4 | 0.001* |
| SROM | 71 | 47.3 | 78 | 52.0 | ||
| Type of vaginal delivery | ||||||
| Normal | 86 | 57.3 | 67 | 44.7 | X2 = 7.42 | 0.001* |
| With episiotomy | 0 | 0.0 | 3 | 1.0 | ||
| With 1st degree of perineal tear | 49 | 32.7 | 32 | 21.3 | ||
| With 2nd degree of perineal tear | 15 | 10.0 | 47 | 32.7 | ||
| Ventose delivery | 0 | 0.0 | 1 | 0.3 | ||
In addition, Table 7 shows that the mean score satisfaction with the assumed position was higher among the experimental group (4.03 ± 0.365) than among the comparison group (2.63 ± 1.303), reflecting a statistically significant difference (t298 = 13.01, p = 0.001). Additionally, the mean score for preference of the assumed position in the subsequent childbirth was higher in the experimental group (4.32 ± 0.771) than in the comparison group (2.63 ± 0.628), with a statistically significant difference (t298 = 21.77, p = 0.001).
| Maternal satisfaction with the assumed position | Experiment group | Comparison group | Independent t-test | df | p-value | ||
|---|---|---|---|---|---|---|---|
| n | Mean ± SD | n | Mean ± SD | ||||
| Level of satisfaction | 150 | 4.03 ± 0.365 | 150 | 2.63 ± 1.303 | 13.01 | 298 | 0.001 * |
| Position preference in the next childbirth | 150 | 4.32 ± 0.771 | 150 | 2.63 ± 0.628 | 21.77 | 298 | 0.001 * |
Discussion
Findings revealed that participants in both groups were demographically homogeneous, with no statistically significant differences. These results correspond with the outcomes of an observational cohort study conducted by Gizzo et al. (2014) and a quasi-experimental study by Emam and Al-Zahrani (2018) to compare the impacts of recumbent and alternative positions on childbirth progress, mode of delivery, and neonatal well-being. In addition, the findings revealed no substantial differences between both groups in relation to age, educational level, nationality, residence, and occupation. This uniformity among the experiment groups helps reduce extraneous factors, which may interrupt the accuracy of measuring the effects of the planned intervention on the childbirth process and outcome.
We discuss the findings based on the labor outcomes: childbirth progress, duration of childbirth, mode of delivery, maternal satisfaction, and level of pain.
Childbirth progress. The mean duration of uterine contractions was higher among participants in the experimental group than among the participants in the comparison group, with statistically significant differences between the participant groups. Similarly, in an Egyptian study, Emam and Al-Zahrani (2018) reported an upright position’s positive effect on childbirth progress. These might be related to the effect of gravity in an upright position on preventing aortocaval squeezing and thereby strengthening uterine contractions. Also, the findings of our study revealed a high statistically significant difference in cervical dilatation between the two groups. Likewise, previous studies by Gizzo et al. (2014) and Chaillet et al. (2014) found that women in the upright position group showed better progress in cervical dilatation than those in the recumbent position group after the first, second, and third hours of assuming the position. These results may be attributed to the fact that upright positions such as sitting, standing, and kneeling during the first stage of childbirth enable the abdominal wall to relax, thereby enabling gravity to pull the uterine fundus forward. In addition, concerning the fetal head descent, the present study found a significant difference between the two groups at the first, second, and third hours of childbirth after assuming the position. Similarly, Gizzo et al. (2014) and Emam and Al-Zahrani (2018) revealed that upright positions aid in bringing the fetus down into the birth canal with the help of gravity. That is probably because upright positions strengthen the pelvic muscles and expand the pelvic area, which improves fetal descent.
Duration of childbirth. The current study’s findings align with Berta et al. (2019) study, which investigated the effect of maternal birth positions on the duration of the second stage of childbirth by conducting a systematic review and meta-analysis of databases. They reported a reduction in the duration of the second stage of birth among women in a relaxed sacrum birthing position. In addition, these findings are consistent with previous studies (Walker et al., 2018; Zaky, 2016), which reported that women in the upright position group had a significantly shorter duration of the first, second, and third stages of childbirth than women in the other group. Furthermore, it was suggested that women who assumed upright had a shorter childbirth duration by 1 hour and 22 minutes than women who assumed the recumbent position. They justified these findings by referring to changing maternal position, frequently moving the pelvic bones, and assisting the fetal descent into the pelvic canal. In contrast, Huang et al. (2019) reported that the upright posture during the first stage of childbirth did not shorten childbirth duration.
Mode of delivery. The current study showed that most participants in the experiment group had normal vaginal delivery compared to a quarter of the participants in the comparison group. Among the participants in the comparison group, one woman had a ventouse delivery because of delayed progress in cervical dilatation and poor maternal effort. Similarly, in two previous studies by Emam and Al-Zahrani (2018) and Deliktas and Kukulu (2018), the majority of women who assumed upright positions in the first stage of childbirth had a normal vaginal delivery, and one-tenth had forceps and ventouse deliveries in the recumbent position group compared to no one in the upright position group. On the other hand, a study by Ibrahim et al. (2020) found no significant difference between women assigned to upright versus recumbent positions for the mode of delivery and duration of the second and third stages of childbirth.
Maternal satisfaction. The present study finding revealed that participants in the experiment group were more satisfied than those in the comparison group, with a statistically significant difference. The study results are consistent with the findings of studies by Deliktas and Kukulu (2018) and Johnson et al. (2017), who examined the effectiveness of ambulation during the first stage of childbirth on the outcomes of delivery among primigravida women and found that mothers who stayed in bed and did not walk around had lower satisfaction with childbirth than mothers who walked around or moved from one place to another. Similarly, studies by Bohren et al. (2017) and Mathew et al. (2012) reported that women who were allowed to assume an upright posture were more satisfied and secure in childbirth than women who stayed in bed and did not walk around. In the same perspective, a randomized controlled trial conducted by Barasinski et al. (2018) to evaluate the effect of an upright position during the first stage of childbirth on parturients’ satisfaction indicated that women in both groups preferred the upright posture. Additionally, Al-Seady et al. (2017) assessed the effect of the upright versus recumbent positions during the active phase of the first stage of childbirth outcomes. Their study revealed that those in the upright position group had higher satisfaction scores than those in the recumbent position group. Moreover, Huang et al. (2019) and Mathew et al. (2012) reported that the upright posture during the first stage of childbirth was a safe and well-accepted alternative for women.
Level of pain. There was a high statistically significant difference between the study and comparison groups in the first, second, third, and fourth hours after assuming the chosen position in relation to pain level. These findings are similar to those of previous studies (Emam & Al-Zahrani, 2018; Shenbagavalli & Menaka, 2016). The justification for this may be that movement can minimize the pain’s severity; thus, it was recommended that the woman move freely and respond to her body’s signals for mobilization and position modification during childbirth. Moreover, Shenbagavalli and Menaka (2016) revealed that breathing exercises, massage, and position modifications were effective in reducing maternal pain during the first stage of childbirth.
Implications of the Study
With the findings of the current study, some recommendations were developed, including: First, educational programs for midwives and nurses on the different delivery positions, as well as the impacts of each, are essential to enable them to offer appropriate advice to childbirth women and improve intrapartum care. Second, assuming upright positions during the first stage of childbirth must be recommended to all women after explaining the benefits of each one. Third, laboring women must be supported in making an informed choice for their birthing position for a better childbirth experience and satisfaction. Fourth, increasing community awareness by developing orientation and education programs regarding delivery preparation through variable platforms. Fifth, further research studies and systematic reviews can be conducted with adequate attention to other possible delivery positions and integrating neonatal outcomes. Moreover, assess the nurses’ and midwives’ knowledge, attitudes, practices, and barriers to applying for different positions during the first stage of childbirth.
Limitations of the Study
The main limitation was the extension period for data collection due to the COVID-19 pandemic in the summer of 2020. However, these limitations did not affect the accuracy of the results.
Conclusion
Based on the findings of the current study, it can be concluded that assuming an upright position during the first stage of childbirth has benefits for a laboring woman by significantly improving childbirth progress, shortening the duration of the three stages of birth, reducing the level of pain, increasing maternal satisfaction with childbirth.