









Background
Gestational Diabetes Mellitus (GDM) is a common health condition diagnosed irrespective of income country status and has been reported as an increasing trend in the past 20 years (Bahram Mohebbi et al., 2019; Carolan-OIah, 2016; Rollo et al., 2020). GDM is often related to maternal and fetal complications because of maternal hyperglycemia, one of the primary predictors of maternal-fetal complications (Borgen et al., 2019; Lefkovits et al., 2019). Maternal complications of GDM include preeclampsia and birth trauma, while in the fetus, it can cause macrosomia, shoulder dystocia, intrauterine death, and stillbirth (Carolan-Olah et al., 2017a; Lefkovits et al., 2019; Mustad et al., 2020; Rasekaba et al., 2016).
Health empowerment intervention strategies may improve glucose levels for mothers with GDM to reduce the risk of complications (Borgen et al., 2017; Lefkovits et al., 2019; Mirfeizi M, 2017; Rollo et al., 2016). Several studies have found that blood glucose monitoring and lifestyle modifications, such as glucose, improve health outcomes without complications (Allehdan et al., 2019; Carolan-Olah & Sayakhot, 2019; Kennelly et al., 2016; Sayakhot et al., 2016). Nevertheless, these approaches are challenging for women with GDM because they require learning and adopting self-care skills in a short time (American Diabetes Association, 2019).
The self-care has been defined as an individual’s, family’s, and community’s ability to improve and sustain well-being, avoid diseases and cope with the health-related condition themselves or with the assistance of a healthcare provider (Carolan-OIah, 2016; Lefkovits et al., 2019). Self-care is an essential component of health empowerment and has been used for GDM management in preventing maternal and fetal complications (Mohebbi et al., 2019). In addition, the World Health Organization (WHO) also recommends that women recognize their potential for safer pregnancy (Carolan-OIah, 2016). In GDM management, health education intervention is an essential component of self-care to train self-care skills, blood glucose monitoring, behavioral change, healthy lifestyle, decision-making, and others (Carolan-OIah, 2016; Ge et al., 2016; Hussain et al., 2015; Kusumaningrum et al., 2022; Tavakkoli et al., 2018; Wah et al., 2019).
Therefore, it is imperative to produce a GDM health education intervention package to improve the quality of health services and strengthen individual self-care skills. The content of the GDM package should be simple, comprehensible, accessible, and interesting for women with GDM. The model framework for the development of educational packages commonly uses the CIPP (context, input, process, and product) model for intervention evaluation and data extraction. The CIPP is widely used for the review of programs or projects and was developed to provide systematic information for decision-making and proactive evaluation (Aziz et al., 2018). However, limited studies use the CIPP model. Therefore, a systematic literature review on GDM education is essential for guiding the development of health education packages. The present study aimed to identify self-care domains, approaches, and techniques for a self-care educational guide package for women with GDM appropriate for their country and culture.
Methods
Search Strategy
A systematic review of original research using a quantitative or qualitative study method on GDM education was conducted. The protocol was registered in PROSPERO under the scope for synthesis without meta-analyses (SWiM) (Campbell et al., 2020). Published data were obtained from Web of Science, Scopus, and Ovid electronic databases. The review search was based on TITLE-ABS-KEY (development OR develop OR developing) AND (health education package OR health education module OR health education intervention OR health teaching OR health intervention OR self-management OR self-intervention) AND (control of glucose level OR glucose management OR glycaemic control OR glycaemic management) AND (Gestational Diabetes Mellitus OR diabetes in pregnancy OR pregnant women with diabetes) (see supplementary file).
Selection of Studies
A list of titles selected was screened, and relevant abstracts were assessed based on the inclusion criteria: a journal article, written in English, and published between 1 January 2016 and 19 December 2022. The PICO model was used that covers the targeted population, type of intervention, a comparative group for intervention, and study outcomes (Table 1).
| Acronym | Definition | Description |
|---|---|---|
| P | Patient and problem | Inclusion criteria: Pregnant women with GDM at 20 to 36 weeks of gestation. The exclusion criteria were women with pre-gestational and diabetes type 1 or 2 |
| I | Intervention | Education materials or programs for women with GDM |
| C | Control or comparison | Only received standard care, no intervention or another intervention |
| O | Outcome | Effective and not effective assessment |
Data Extraction
The criteria used in the CIPP model can be defined in various ways depending on the program assessment by multidiscipline (Lee et al., 2019). In this present study, data extraction utilized a standardized CIPP model (supplementary file), which was performed by the first authors (ZH and RS) and reviewed by the second author (RS) to verify the extracted data.
Quality Appraisal Assessment
Extracted relevant literature was assessed using the Mixed Methods Appraisal Tool (MMAT) (Hong et al., 2018). Five research designs were included in the MMAT for quality appraisal assessment, as shown in Table 2 (randomized controlled trials), Table 3 (non-randomized controlled trials), Table 4 (qualitative studies), and Table 5 (mixed-methods study). The MMAT enables researchers to critically select quality empirical studies through a proper risk of bias screening based on the study methodology reported. This quality appraisal eliminated non-empirical papers, including review articles and theoretical papers, from being included in this study.
| Criteria | (Rasmussen et al., 2020) | (Zandinava et al., 2017) | (Mackillop et al., 2018) | (Kolivand et al., 2019) | (Al-Ofi et al., 2019) | (Guo et al., 2019) | (Mirghafourvand et al., 2019) | (Gharachourlo et al., 2018) | (Ammulu et al., 2019) | (Tian et al., 2021) | (He et al., 2022) | (Xie et al., 2022) |
|---|---|---|---|---|---|---|---|---|---|---|---|---|
| Clear research question (s) | Yes | Yes | Yes | Yes | Yes | Yes | Yes | Yes | Yes | Yes | Yes | Yes |
| Collected data addresses the research questions | Yes | Yes | Yes | Yes | Yes | Yes | Yes | Yes | Yes | Yes | Yes | Yes |
| Randomization appropriately performed | Yes | Yes | Yes | Yes | Yes | Yes | Yes | Yes | Yes | Yes | Yes | Yes |
| The groups comparable at baseline | Yes | Yes | Yes | Yes | Yes | Yes | Yes | Yes | Yes | Yes | Yes | Yes |
| Complete outcome data | Yes | Yes | Yes | Yes | Yes | Yes | Yes | Yes | Yes | Yes | Yes | Yes |
| Outcome assessors blinded to the intervention provided | Yes | Yes | Yes | Yes | Yes | Yes | Yes | Yes | No | Yes | Yes | Yes |
| Participants adhere to the assigned intervention | Yes | Yes | Yes | Yes | Yes | Yes | Yes | Yes | Yes | Yes | Yes | Yes |
| Criteria | (Mohebbi et al., 2019) | (Kim et al., 2019) | (Al-Hashmi et al., 2018) | (Rokni et al., 2022) |
|---|---|---|---|---|
| Clear research question(s) | Yes | Yes | Yes | Yes |
| Collected data addresses the research questions | Yes | Yes | Yes | Yes |
| Participants representative of the target population | Yes | Yes | No | Yes |
| Measurements appropriate regarding both the outcome and intervention (or exposure | Yes | Yes | No | Yes |
| Complete outcome data | Yes | Yes | Yes | Yes |
| Confounders accounted for in the design and analysis? | Yes | Yes | Yes | No |
| During study period, intervention administered (or exposure occurred) as intended | Yes | Yes | Yes | Yes |
| Criteria | (Skar et al., 2018) | (Carolan-Olah & Sayakhot, 2019) |
|---|---|---|
| Clear research question(s) | Yes | Yes |
| Collected data addresses the research questions | Yes | Yes |
| Qualitative approach is appropriate to answer the research question | Yes | Yes |
| Qualitative data collection methods adequate to address the research question | Yes | Yes |
| Findings adequately derived from the data | Yes | Yes |
| The interpretation of results sufficiently substantiated by data | Yes | Yes |
| Coherence between qualitative data sources, collection, analysis, and interpretation | Yes | Yes |
| Criteria | (Surendran et al., 2021) |
|---|---|
| Clear research question(s) | Yes |
| Collected data addresses the research questions | Yes |
| Is there an adequate rationale for using a mixed-method design to address the research question? | Yes |
| Are the different components of the study effectively integrated to answer the research question? | Yes |
| Are the outputs of the integration of qualitative and quantitative components adequately interpreted? | Yes |
| Are divergences and inconsistencies between quantitative and qualitative results adequately addressed? | Yes |
| Do the different components of the study adhere to the quality criteria of each tradition of the methods involved? | No |
The authors followed the MMAT guideline for quality appraisal assessment using three main steps. Firstly, both authors (ZH and RS) independently assessed articles retrieved for quality appraisal and reached a consensus for an agreement. All eligible studies were evaluated based on the two initial MMAT screening questions: (1) Are there clear research questions? and (2) Do the collected data allow us to address the research question? If the answer to one or both questions is "No" or "Can't tell," it was assumed that the paper
was not an empirical study and could not be evaluated further. Secondly, the relevant category of the study was selected to assess the description of the conduct of the study based on the criteria listed in the MMAT. The criteria respect the distinctive methodological qualities unique to each component utilized. Thirdly, each study design was evaluated in meeting the criteria by indicating “Yes,” “No,” or “Can’t Tell”. If the criteria were not satisfied, it would be indicated by the letter “No.” Finally, the other authors (ZAM and RZ) came in when disagreements between the 1st and 2nd authors were not obtained.
Data Analysis
Content analysis with the CIPP model and Atlas Ti version 8.0 software was employed to summarize the specific data garnered from the studies, and the findings were tabulated. This method was applied in this review, given its capacity to extract qualitative and quantitative data for analyses (Aziz et al., 2018).
Results
Characteristics of Included Studies
Figure 1 shows the process of reviewing evidence from three main web databases. There were 5878 articles identified from the databases, and 4,897 articles remained after the exclusion of the duplicate articles. The titles and abstracts of these articles were then reviewed to eliminate papers irrelevant to the research objectives. Finally, the full texts of the presumably relevant articles along with their references were screened. Only 19 articles were found to be pertinent to this study.
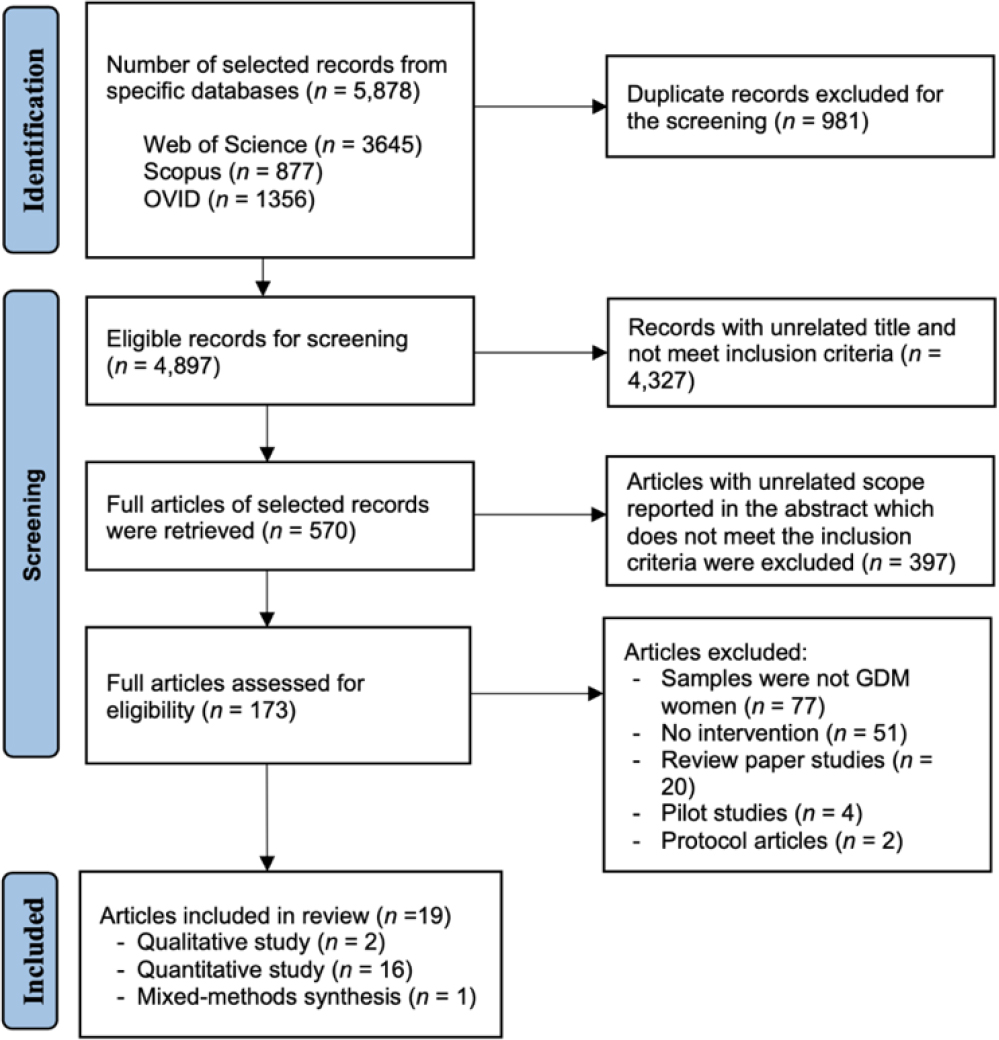
The 19 articles were assessed and summarized based on the CIPP model and finally reported the findings according to the SWiM checklist (Campbell et al., 2020) (supplementary file). Only sixteen quantitative studies, two qualitative and one mixed-methods study, were included.
There were twelve randomized control trials (RCT) (Al-Ofi et al., 2019; Ammulu et al., 2019; Gharachourlo et al., 2018; Guo et al., 2019; He et al., 2022; Johnson & Berry, 2018; Kolivand et al., 2019; Mackillop et al., 2018; Mirghafourvand et al., 2019; Rasmussen et al., 2020; Tian et al., 2021; Xie et al., 2022; Zandinava et al., 2017), four quasi-experimental (Al-Hashmi et al., 2018; Kim et al., 2019; Mohebbi et al., 2019; Rokni et al., 2022), two interpretative phenomenological analysis (IPA) designs (Carolan-Olah et al., 2017b; Skar et al., 2018), and one mixed-methods study (Surendran et al., 2021) Only three studies applied theory in their research, and all used the Health Belief Model (Mohebbi et al., 2019; Skar et al., 2018; Surendran et al., 2021). This review identified 2,237 women with GDM (1108 in the intervention group, 1094 in the control group, and 35 in the qualitative).
Results of Quality Appraisals
The results of quality appraisals of this present study are shown in Table 2 to Table 5.
Results of Content Analysis Identifying self-care domains
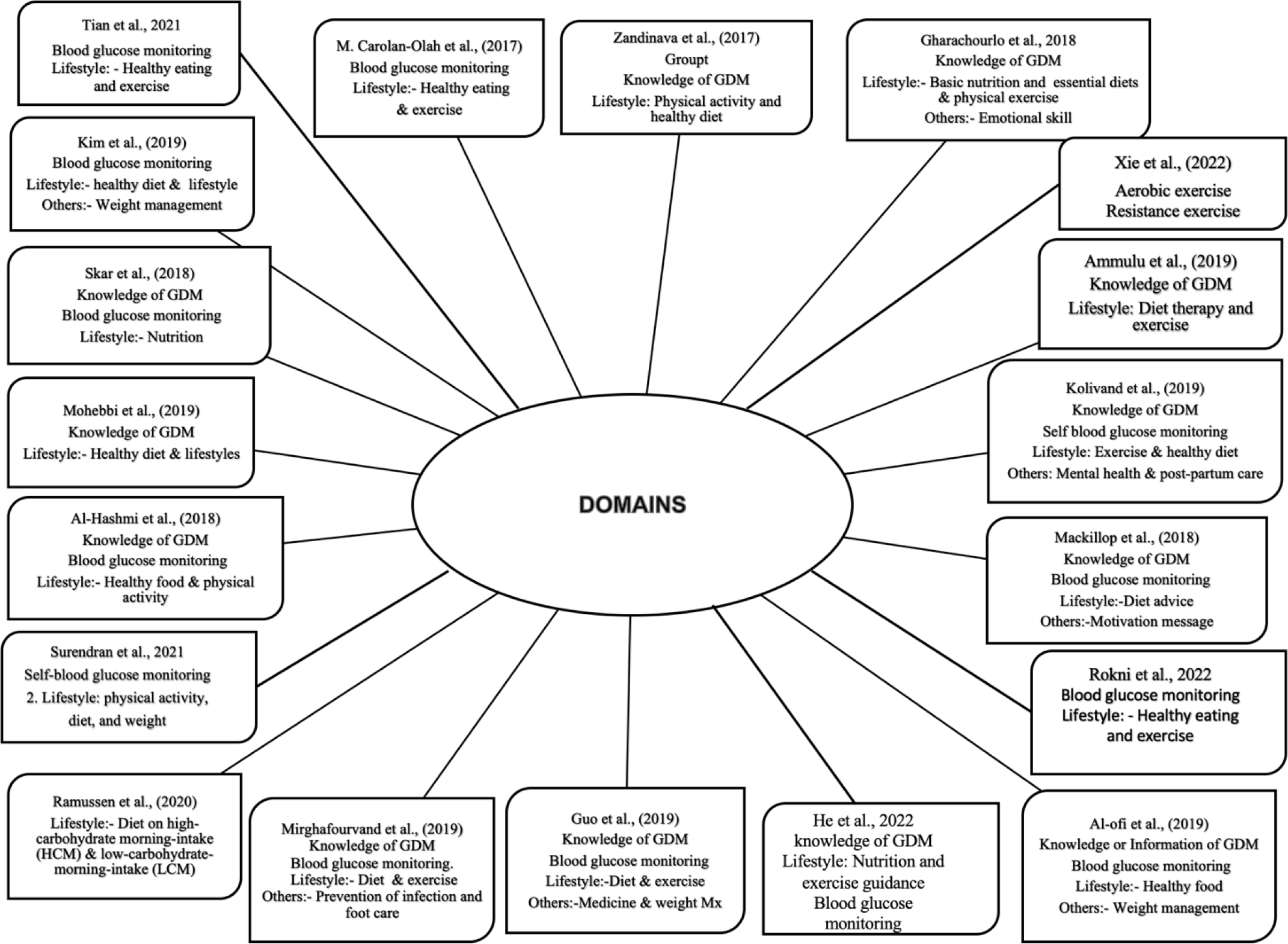
Four main domain groups of intervention for GDM self-care: (1) knowledge or Information about GDM, (2) blood glucose monitoring, (3) healthy lifestyle (healthy diet or nutrition and exercise or physical activity), and (4) others (Figure 2).
(1) Knowledge information on GDM
A total of 12 articles (about half of the total articles reviewed) applied the knowledge or information on the GDM domain in their intervention (Al-Hashmi et al., 2018; Al-Ofi et al., 2019; Ammulu et al., 2019; Guo et al., 2019; He et al., 2022; Kolivand et al., 2019; Mackillop et al., 2018; Mohebbi et al., 2019; Skar et al., 2018; Tavakkoli et al., 2018; Zandinava et al., 2017). Knowledge or information on GDM includes the definition, causes, symptoms, treatment, and complications of GDM on the mother and fetus and their prevention. Only two studies provided knowledge and education on insulin, including self-injection, using a model (Kolivand et al., 2019; Tavakkoli et al., 2018). Consequently, higher scores for self-efficacy and pregnancy outcomes were observed in the intervention groups (Mackillop et al., 2018), which significantly improved their lifestyle (Tavakkoli et al., 2018). All studies that implemented this domain positively impacted the outcomes evaluated.
Most of the activity strategy for the educational session was delivered through various teaching methods, such as lectures, PowerPoint presentations, and videos, and only one study applied role play (Mohebbi et al., 2019). Participants were allowed to ask questions at the end of the education session, which were answered by the educator. While strategy setting an achievable goal and motivational message were used by the studies applied HBM (Al-Hashmi et al., 2018; Mohebbi et al., 2019; Surendran et al., 2021) to enhance self-efficacy.
The duration of the intervention varies between one and multiple sessions, ranging from 30 to 60 minutes in every session. All knowledge on GDM was delivered directly to the participants except for one study (Mohebbi et al., 2019) that encouraged family involvement for social support to motivate encouragement, empathy, concern, or caring. The majority of the education session delivered by nurses or nurse-midwifery or researchers, and two studies (Mohebbi et al., 2019; Zandinava et al., 2017) did not mention who gave the education session.
(2) Blood glucose monitoring
Ten studies monitored fasting blood glucose (FBG) and one or two hours postprandial (Al-Ofi et al., 2019; Guo et al., 2019; He et al., 2022; Kim et al., 2019; Kolivand et al., 2019; Rasmussen et al., 2020; Rokni et al., 2022; Tian et al., 2021; Xie et al., 2022; Zandinava et al., 2017), whereas only five studies measured hemoglobin A1c (HbA1c) (Al-Ofi et al., 2019; Guo et al., 2019; Kim et al., 2019; Mackillop et al., 2018; Mohebbi et al., 2019).
FBG was reported to be significant in six studies (Guo et al., 2019; He et al., 2022; Rasmussen et al., 2020; Rokni et al., 2022; Tian et al., 2021; Xie et al., 2022), while four studies found it significant for the one hour or two-hour postprandial blood glucose assessment (Al-Ofi et al., 2019; Guo et al., 2019; Kolivand et al., 2019; Zandinava et al., 2017). While three studies found HbAIc to be significant (Guo et al., 2019; Kim et al., 2019; Mohebbi et al., 2019), another two found it to be not significant but decreased in mean (Al-Ofi et al., 2019; Mackillop et al., 2018).
Only five articles reported activity strategies to assess glucose levels using a routine monitoring system. Another five studies used either mobile apps or telemedicine for glucose level measurement and monitoring (Al-Ofi et al., 2019; Guo et al., 2019; Mackillop et al., 2018; Rokni et al., 2022; Skar et al., 2018) while WeChat was employed in two studies (He et al., 2022; Tian et al., 2021).
In most articles, the duration of monitoring blood glucose levels ranges from four to six weeks at weekly intervals, whereas only Mohebbi et al. (2019) recorded a monitoring period between 3 and 10 months. The activity target for blood glucose monitoring is to get the participant to adhere to the behavior changes and control the glucose level.
In terms of activity strategies, the main target for monitoring blood glucose levels was for the participant to stick to the recommended behavioral changes for optimal control. A comparative study between mobile application blood glucose management systems and clinic standard care monitoring that served as an alerting system also emphasized hypoglycemia or hyperglycemia in their education (Mackillop et al., 2018). Therefore, any type of application is crucial to alert women with GDM about their health status. In most studies, either a nurse or nurse-midwifery was responsible for teaching the participants how to practice self-blood glucose monitoring.
(3) Healthy lifestyle
Healthy diet or nutrition
All articles reviewed had diet or nutrition as a self-care intervention. Nevertheless, the studies focused solely on exchanging carbohydrates and none on the involvement of the glycaemic index concept. Only one study emphasized high energy content and carbohydrate for morning intake and low evening intake and kept glucose levels measured four times a day (Rasmussen et al., 2020). The study showed that the group with high carbohydrate intake in the morning had better glucose level control and improved insulin sensitivity.
A dietician delivered an education session for nutrition activity strategies and a healthy diet. Different techniques, such as nutrition classes or direct teaching, were used in the process, and most sessions were individualized. One to four educational sessions were performed, with each session ranging from 30 to 45 minutes. The findings from this review disclosed the significance for participants and dieticians to reach an agreement regarding the daily calorie intake as per the standard GDM guidelines. This activity aims to bring the glucose level to the normal range by following the recommended menu.
Exercise and physical activity
This domain was applied the most as a self-care education package intervention in this review (Al-Hashmi et al., 2018; Ammulu et al., 2019; Carolan-Olah et al., 2017b; Kim et al., 2019; Kolivand et al., 2019; Mirghafourvand et al., 2019; Mohebbi et al., 2019; Tavakkoli et al., 2018; Zandinava et al., 2017). Exercise or physical activity showed positive outcomes and was able to modify the participants’ lifestyles to become healthier. However, only one study demonstrated no impact on the participants’ quality of life, contrary to other studies that proved exercise or physical activity effectively improved quality of life when the same parameters were examined (Zandinava et al., 2017).
Motivational counseling is vital to promote self-efficacy among participants without interruption throughout the sessions (Ammulu et al., 2019; Kim et al., 2019; Tavakkoli et al., 2018). Generally, education sessions for motivational counseling using video, counseling, and role-playing as the teaching methods lasted from 30 to 45 minutes. The present review depicted that it takes approximately two to four weeks to complete the education session for the activity.
Nevertheless, Kim et al. (2019) demonstrated the efficacy of using the website approach to monitor the exercise pattern among participants. In the study, the nurses placed a phone call to serve as a reminder for participants to perform the exercise and achieve the targeted goal (Rokni et al., 2022).
(4) Other domains
Mental health and emotional support
Three studies reported on mental health education (He et al., 2022; Kolivand et al., 2019; Tavakkoli et al., 2018), and only a study specified the importance of emotional skill training (Tavakkoli et al., 2018). The factors evaluated were blood anxiety, depression score, glucose level, self-efficacy, lifestyle, and pregnancy outcome. The study’s findings revealed that women with GDM in the intervention group had better anxiety levels and lifestyle, decreased mean glucose levels, significant self-efficacy, as well as better neonatal outcomes.
We have discovered that activity strategy for emotional skills (Tavakkoli et al., 2018), coping strategies, and follow-up (He et al., 2022) in GDM at any level of health literacy rise with good communication skills and counseling. Therefore, counseling techniques using lectures, PowerPoint presentations, role-playing, and individualized or focus group discussions specifically on “healthy lifestyle” were commonly employed throughout educational sessions.
The duration of the counseling reported for one session ranges between 30 - 40 minutes, and the number of sessions is divided into two to three sessions. Counseling strategies should be emphasized on basic nutrition education, essential diets, awareness of the adverse effects of nutrition on health status, and the importance of regular physical activities in improving self-care. The counseling can be delivered by a trained nurse and nutritionist.
Weight management
Only three studies included this domain in the intervention, and they measured FBG, two hours postprandial, and HbAIc (Al-Ofi et al., 2019; Guo et al., 2019; Kim et al., 2019) besides other outcomes. The finding revealed significant differences for FBG, one or two hours postprandial (Al-Ofi et al., 2019; Guo et al., 2019), and only one study showed a significant difference in weight management (Al-Ofi et al., 2019).
Approaches and techniques
Most of the interventional studies used a face-to-face educational group session approach. Seven studies provided booklets or pamphlets as educational materials (Al-Hashmi et al., 2018; Kolivand et al., 2019; Mirghafourvand et al., 2019; Rasmussen et al., 2020; Rokni et al., 2022; Tavakkoli et al., 2018; Zandinava et al., 2017), while six studies used mobile applications (Al-Ofi et al., 2019; Guo et al., 2019; Mackillop et al., 2018; Skar et al., 2018; Surendran et al., 2021), two studies used WeChat (He et al., 2022; Tian et al., 2021), one study used web-based (Kim et al., 2019) and two studies applied counseling sessions (Ammulu et al., 2019; Kim et al., 2019) as shown in Figure 3. Most of the studies assessed participants four weeks after intervention. Two studies performed assessments six weeks after delivery, whereas one study conducted assessments three and six months after the intervention, and four other studies implemented baseline assessments (supplementary file).

There were two studies (Ammulu et al., 2019; Kim et al., 2019) focused on counseling strategies to improve the lifestyles of respondents by measuring the quality of life (Ammulu et al., 2019), health literacy, and lifestyle scores (Kim et al., 2019). Both studies aimed for healthy lifestyle changes via the sub-domains of knowledge on coping with GDM; communication skills; physical exercise; psychological, diet therapy; pharmacological and emotional skills. Counseling intervention was performed in groups, and it concluded that counseling by midwives significantly helped mothers with GDM to modify their unhealthy lifestyles and increase health literacy (Tavakkoli et al., 2018). In agreement, another study demonstrated a positive impact on the management of GDM after conducting counseling sessions at baseline and one-month post-intervention (Mohebbi et al., 2019). In contrast, only three studies applied a theory in their health education training and used the Health Belief Model (Mohebbi et al., 2019; Skar et al., 2018; Surendran et al., 2021). Most of the findings and evidence revealed that nurses and midwifery nurses were mainly responsible for delivering most educational interventions.
Discussion
Identifying Self-Care Domains
In this review, 19 articles were assessed and summarized based on the CIPP model. The present study identified four main domain groups of intervention for GDM self-care: (1) knowledge or Information about GDM, (2) blood glucose monitoring, (3) healthy lifestyle (healthy diet or nutrition and exercise or physical activity), and (4) others.
Several studies showed that pregnant women with GDM who had less knowledge of GDM had higher blood glucose levels and a poorer attitude towards self-care compared to pregnant women with GDM who had good knowledge or information about the condition (Ge et al., 2016; Hussain et al., 2015; Mensah et al., 2019). Therefore, women with GDM recommend having a good understanding of the disease once diagnosed because knowledge will allow an individual to process and use the information to guide health decisions, which has been a major concern in those studies (Bhowmik et al., 2018; Liu et al., 2020; Muhwava et al., 2019). It also focused on understanding health information in everyday situations, such as healthy behaviors, healthy lifestyles, and health terms (Hussain et al., 2015; Liu et al., 2020).
In addition, the studies showed that participants were likely to have received information on the risk of GDM complications in the fetus, which may have encouraged adherence to GDM self-care plans (Al Hashmi et al., 2022; Kennelly et al., 2016). Hence, delivering GDM knowledge to pregnant women with GDM through self-care health education should be considered a vital intervention domain. Women with GDM can improve their self-care abilities with adequate treatment and education (Mirfeizi M, 2017; Mohanty et al., 2020) as health education is an essential component in addressing major health concerns such as maternal and infant mortality, and healthy life promotion programs (Bhowmik et al., 2018; Draffin et al., 2017; Muhwava et al., 2019). Currently, self-care education has progressed from a purely educational and passive approach to one that emphasizes empowerment, decision-making skills, and self-care, and WHO suggests it (World Health Organization, 2019). All pregnant women with diabetes should begin self-care education and support as soon as diabetes is diagnosed (Crawford, 2017).
However, glucose measurements such as FBS, postprandial, and HbA1c were not significantly different between the groups (intervention and control) in all the articles reviewed. These findings were contrary to the previous integrative review of educational and interventional programs for GDM management (Carolan-OIah, 2016). The inconsistency may be due to participants’ poor compliance with the management or the intervention introduced. Nevertheless, this hypothesis cannot be confirmed as only one study demonstrated good compliance and ideal blood glucose results following the intervention.
Apart from that, all studies emphasized healthy eating or carbohydrate exchange, but none of these reviews mentioned the Glycaemic Index (GI) concept. GI is a scale that ranks carbohydrates in different diets based on their impact on postprandial glucose response; foods with a high GI caused more substantial blood glucose swings than those with a lower GI (Anuar et al., 2020). Studies showed that without limiting dietary carbs, low-GI dietary treatments reduced the postprandial blood glucose and the number of insulin demands in women with GDM (Anuar et al., 2020; Carolan-OIah, 2016; Lefkovits et al., 2019). Furthermore, the Cochrane review (Han et al., 2017) and other studies recommended that women with GDM should be emphasized that foods with a low GI should be substituted for items with a high GI (Anuar et al., 2020; Brown et al., 2017; Crawford, 2017; Hasbullah et al., 2020). Therefore, besides the carbohydrate exchange, the addition of the GI concept is recommended in the future development of self-care educational intervention packages for GDM based on the culture and settings.
In this review, exercise and physical activity have been the most used self-care education package interventions and demonstrated a positive impact on glycaemic control and pregnancy outcome (Al-Hashmi et al., 2018; Ammulu et al., 2019; Carolan-Olah et al., 2017b; Kim et al., 2019; Kolivand et al., 2019; Mirghafourvand et al., 2019; Tavakkoli et al., 2018; Zandinava et al., 2017). Increasing awareness regarding exercise or PA will lead to improved individual self-care and higher quality of life (Anjana et al., 2016; Gilbert et al., 2019; Mohanty et al., 2020; Pinidiyapathirage et al., 2018).
However, Cochrane updates and the NICE Guideline reported that when compared to routine antenatal care, exercise programs such as individualized exercise with regular advice, weekly supervised group exercise sessions, or home-based stationary cycling, either supervised or unsupervised, had no discernible effect on improving insulin sensitivities (Brown et al., 2017). On the contrary, an integrated review concluded that increased activity levels are most effective at lowering maternal blood glucose levels and insulin requirements during pregnancy (Carolan-OIah, 2016). Therefore, we suggest that exercise or physical activity in self-care among mothers with GDM should be studied to indicate whether it is effective in controlling GDM or inversely to fill the gap in this review.
Approaches and Techniques
Most of the studies in this review used group training sessions, which had a better impact on the respondents, thus proving that the group approach is more effective than individual sessions in health education (Kolivand et al., 2019; Mirghafourvand et al., 2019; Mohebbi et al., 2019; Rasmussen et al., 2020; Tavakkoli et al., 2018; Zandinava et al., 2017). Besides, most studies approached participants between 24 to 28 weeks of gestation. Unlike other types of diabetes, GDM recedes after childbirth. Therefore, self-care education must be carried out intensively to enhance self-care for women with GDM to achieve well-controlled glucose levels and produce good pregnancy outcomes(Mensah et al., 2019; Wah et al., 2019).
In this review, we have found that various educational intervention strategies are used in managing GDM. Almost all the studies analyzed reported combination interventions, combining multiple interventions to treat GDM. The combination of input for the self-care education intervention covers knowledge of GDM, physical activity, nutrition, self-management education intervention, glucose monitoring, and practicing healthy eating.
The majority of the educational intervention was delivered by nurses or midwifery nurses. A study on diabetes awareness among the public in Malaysia found that respondents who received information from medical practitioners showed a better understanding compared to getting information from other sources such as internet sources, friends, or relatives (Qamar et al., 2017). Furthermore, according to Yong et al. (2018), health education interventions for mothers with GDM from medical practitioners such as nurses were essential to increase knowledge about GDM so they can perform good self-care in managing GDM. This is in line with the recommendations by the WHO (Mensah et al., 2019), where they have recommended that health education be delivered by medical practitioners such as nurses and doctors to improve the quality of self-care in the treatment and management of a disease. Some other researchers in their study found that mothers with GDM who had poor knowledge about GDM experienced higher blood glucose levels compared to mothers with GDM who had good knowledge, and they also showed a bad attitude toward self-care (Ge et al., 2016; Ghasemi et al., 2021; Kolivand et al., 2018).
Three studies were found to apply a theory that used the Health Belief Model (HBM) in their health education training (Mohebbi et al., 2019; Skar et al., 2018; Surendran et al., 2021). Hence, it is suggested to test other behavioral theories to change the behaviors of GDM women toward GDM management. It is essential to understand the patient’s behavior using the behavioral approach to offer guidance on determinants of health behavior and health services (Isa et al., 2017; Lucille S. Eller et al., 2018; Matarese et al., 2018). It can also offer new approaches to nursing practices to improve patient care efficacy (Sleet & Dellinger, 2020). Self-efficacy also may assist patients or mothers with GDM in removing obstacles self-care and adhering to long-term health gains (Yang et al., 2022). Furthermore, good self-efficacy and self-care behaviors in GDM management can help prevent or delay the development of type II diabetes and lower the risk of developing maternal and neonatal type II diabetes in the future (Isa et al., 2017; Mensah et al., 2019).
Implications for Practice
The findings of the present review provided evidence of the benefits of GDM educational and interventional approaches for pregnant women with GDM. A self-care health educational GDM package reviewed was based on four domains. The most preferred method to achieve effectiveness was highlighted as the face-to-face approach. Thus, a combination of face-to-face sessions, digital e-book resources, and printed booklets was employed to enhance usage compliance. In order to assist women with GDM to retain the self-care knowledge gained post-nursing intervention, it is essential to equip them with informational materials that can be easily recalled and utilized as additional reference or guide at home. Providing written health information could also improve the association between healthcare providers and patients. Furthermore, the use of GDM educational intervention in assessing the effectiveness should emphasize the positive effects of self-management in enhancing self-efficacy, higher satisfaction scores, optimal glucose control, monitoring, and better self-care behavior.
The evidence of the present review will be used for future nursing studies in developing a self-care health education package for GDM that covers information about GDM, healthy lifestyles such as healthy eating or diet, and exercise to help in blood glucose control in preventing GDM complications. The package will be prepared as a booklet as suggested and well accepted as positive feedback is given. In addition, the provision of printed educational materials can improve patients’ health literacy and their personal responsibility, motivation, and attitude toward health. Health education intervention is highly recommended in health promotion to increase self-efficacy, a key domain in improving self-care ability, the quality of nursing care, and facilitated shared care approach between client and the health care providers. Aside from that, a previous study on women’s GDM experiences emphasized the significance of creating GDM management as a routine in accordance with the life, values, and goals of the woman, as well as the necessity for the addition of individually customized and cultural relevant information.
Limitations
The use of only English-written papers and the restricted years of publication placed a limitation on this review. Despite that, this review managed to discover valuable findings and information that can be used as materials for the development of future GDM health educational interventions or programs for GDM women.
Conclusion
Self-care education for women with GDM had a positive impact on GDM outcomes. Knowledge or information about GDM, healthy diet, and exercise or physical activity were the most applied domains of intervention. Thus, these domains should be emphasized in the future development of any interventional program for GDM women. This study might also help healthcare providers design self-care interventions for pregnant women with GDM according to individual needs to enhance their self-efficacy. Finally, most of the studies used a face-to-face educational group session approach and demonstrated a positive impact on the management of GDM.