










Background
HIV/AIDS is now considered a chronic disease that can be managed with the new treatment of Highly Active Anti-Retroviral Therapy (HAART) for several more years. As a result, the life expectancy and quality of life for many affected individuals are increasing (Kalomo et al., 2017). The World Health Organization (WHO) has established a plan for achieving an AIDS-free generation through the 90-90-90 target code, but this goal has not yet been accomplished globally. The target aims for 90% of people living with HIV to know their status, 90% of those diagnosed with HIV to receive continuous ARV therapy, and 90% of those receiving ARV therapy to achieve viral suppression (Bajunirwe et al., 2018). Interventions such as improved cognition, volitional counseling, access to ARVs, and the cessation of stigma have been implemented, resulting in decreased infections and improved health for affected individuals (Breckenridge et al., 2019; Ma et al., 2019). However, there is little evidence to suggest that counseling and screening programs are successful in ensuring that all patients are aware of their HIV status, and even when individuals are diagnosed, few attend ARV treatment programs to suppress the virus’s progression as expected (Denison et al., 2020).
In Indonesia, where HIV/AIDS prevalence is at its highest, visible social, economic, and political consequences have affected every household (Putta et al., 2022). The increase in HIV cases among housewives in several regions of Indonesia has resulted in a rise in the number of children exposed to HIV. HIV transmission in children is mainly due to vertical transmission during pregnancy, childbirth, and lactation (Muskat et al., 2016). A child born to an HIV-positive mother requires special care from the womb to the postnatal period. Regular ARV treatment during pregnancy and childbirth and other preventive measures are necessary to prevent HIV transmission from mother to child. The regular treatment effectively suppresses the virus’s growth until the viral load drops below 1000 copies (Landes et al., 2019). The lower the mother’s viral load, the lower the baby’s risk of contracting HIV from the mother. In one study on HIV-exposed infants’ characteristics, Chen et al. (2019) found poor growth among HIV-exposed Chinese infants, including those HIV-uninfected, compared to unexposed, uninfected infants.
Rencken et al. (2022) explain that HIV-exposed babies have lower neurobehavioral functions, which affect their quality of life and ability to develop reciprocal relationships with primary caregivers. This condition may also impact later childhood development, behavior, and mental health. Therefore, infants affected by HIV should be closely monitored, and their autonomic stability, motor control, and social interaction functions should be assessed regularly. Data on cases of HIV-positive children are generally well-recorded as they relate to treatment needs. However, HIV-exposed children born to HIV-infected mothers who are not always HIV-positive are generally not explicitly documented.
Caregivers play a crucial role in the lives of children exposed to HIV, whether they are parents, relatives, adoptive parents, or guardians. Providing guidance and incorporating strategies into their care is vital to mitigate possible long-term adverse effects on their development. In addition, good parenting is essential for children to develop properly. However, the challenges caregivers face can affect their ability to provide optimal care, and HIV-positive caregivers have been found to harm child outcomes (Sherr et al., 2016). Research has shown that children with HIV-positive caregivers or living in HIV-affected households have significantly worse outcomes than those in HIV-free homes.
Caregivers significantly impact the child’s health status, and understanding the care of children exposed to HIV and caregivers’ health and psychosocial conditions indirectly affects the child’s health status. Nurses are part of the healthcare team involved in maintaining and improving the physical and mental health status of caregivers and children. Nursing care would be better if there is a good understanding of the situation and needs of caregivers and children exposed to HIV.
Although studies on caregivers’ experiences caring for HIV-infected children have been conducted widely, research on caregivers’ experiences caring for HIV-exposed children in Indonesia is still limited. Therefore, further studies are necessary to identify programs that improve the well-being of caregivers and children exposed to HIV. Therefore, this study aimed to explore the experiences of caregivers caring for children under five exposed to HIV.
Methods
Study Design
The study utilized a qualitative method with a descriptive phenomenology approach to understanding caregivers’ experiences caring for HIV-exposed children under five. Qualitative research prioritizes meaning and clarity over quantitative study (Davidsen, 2013; Paley, 2017). The phenomenological inquiry aims to elucidate the structure or essence of the lived experience of a phenomenon in the search for the unity of meaning, which is the identification of the essence of a phenomenon. It accurately describes the everyday lived experience (Rose et al., 1995; Streubert & Carpenter, 2011). The design of this study emphasizes the meanings of caregivers’ experiences in caring for children under the age of five. This study included individual and situational experiences and their coping mechanisms for caring for HIV-exposed children under the age of five.
Participants
The study participants were caregivers of HIV-exposed children living in the Jakarta area and its surroundings. The researcher recruited participants who met the criteria using snowball sampling techniques. Participant inclusion criteria were primary caregivers of children under five exposed to HIV who directly cared for children, such as the mother, adoptive father, mother’s sister, and aunt. They were able to communicate verbally and had been caring for children under five exposed to HIV for at least six months.
The number of participants included in the sample was determined by how much information could be gathered. The data collection process was deemed complete when subsequent interviews did not generate any new information because the process had become repetitive. To determine saturation and the necessity to conclude interviews, they were reviewed concurrently and iteratively with data collection to determine whether they were complete. The themes that emerged from the initial analysis of the interviews were seen in variations and relationships with subsequent interviews until data saturation was reached. After interviewing the tenth caregiver, this study achieved data saturation.
Data Collection
The data collection for this study was conducted between September 2021 and July 2022. Due to COVID-19 and social distancing policies, data were collected online via Zoom meeting. At the initial stage of participant recruitment, the researcher communicated with PLHIV assistants in the Jakarta area and its surroundings. The researcher explained the study’s aim and inclusion criteria to the PLHIV assistants, who then contacted caregivers of HIV-exposed toddlers who met the criteria during clinic visits. The researcher then contacted interested caregivers, explained the study’s objectives, benefits, rights of participants, and data collection procedures in writing, and sent the information via a Google form link through the WhatsApp application. Participants who agreed to participate expressed their consent through the same Google form link. Subsequent participants were obtained based on recommendations from previous participants who met the inclusion criteria.
In the next stage, the researcher agreed with the participants on a suitable time for the online interview. The interviews with all participants were conducted online for 40-60 minutes using the Zoom meeting mode. The research team conducted open-ended interviews following the guide and continued with in-depth interviews. Before the interviews, the researcher explained the process and asked for permission to record the interviews. All participants allowed the researcher to record the interviews. The researcher conducted the interviews in a private place using earmuffs and recorded the audio and visual aspects. Following the interviews, debriefing sessions were conducted to ensure that the session had not caused any harm to the participants before disengaging.
Data Analysis
The recorded interviews were listened to prior to verbatim transcription and then re-listened for better understanding. Two Bahasa language experts transcribed the Bahasa interviews back-to-back to maintain meaning before translating them into English. Biographical information was compiled and labeled in a Microsoft Word document. The transcribed interviews and biographical data were given recognizable file names, stored on a flash drive and personal computer (PC) with a password, and made exclusively available to the research team.
During the data collection phase, the researchers manually analyzed the data using Colaizzi’s analysis of phenomenological interviews. The researchers followed the seven iterative phases of Colaizzi’s method (Colaizzi, 1978; Polit & Beck, 2004): 1) they listened to the audio of the interview, transcribed it, and read it several times to grasp the overall message’s meaning; 2) they extracted all significant statements from the transcripts and compiled a comprehensive list; 3) interpretations were derived from all the significant statements provided; 4) the developed meanings were arranged into themes or clusters; 5) the researchers integrated the themes to provide a comprehensive picture of caregivers’ experiences with HIV-positive children under five; 6) they made a decisive and unequivocal declaration regarding the comprehension of this phenomenon, considering the setting and context of the caregiver’s experience caring for HIV-positive children under the age of five. As a result, this became the inherent meaning; 7) the researchers communicated with all caregivers via WhatsApp to confirm the final analysis. The participants did not provide new data during validation. Instead, the researchers used quotations from participants to emphasize points throughout the presentation of the results, and they used code identities (P1-P10) to protect confidentiality and anonymity.
Rigor
To ensure quality and rigor, the researchers followed several steps based on Lincoln and Guba’s parameters, as outlined by Polit and Beck (2004). These steps included peer debriefing, bracketing of prior assumptions, an audit trail, and member checks for all participants. The researchers also explained the setting, participants’ characteristics, and transactions to achieve transferability. This process confirmed that the interview guide phrasing, ability to comprehend, reliability, and accuracy were sufficient to elicit appropriate responses for the phenomenon.
Ethical Considerations
This study was reviewed and approved by the Commission of Ethics of the Faculty of Nursing, Universitas Indonesia, with an ethics review passing the number of Ket-217/UN2.F12.D1.2.1/PPM.00.02/2021. The researchers initiated contact with all participants through an online chat platform and introduced themselves and the purpose of the study. After the participants understood the research, they expressed their approval to participate in the research through a Google form.
Results
Table 1 shows all ten caregivers who directly take care of children under the age of five. A total of 10 caregivers were involved in this study, comprising nine female caregivers and one male caregiver. Seven of them were mothers who were HIV positive, one was an adoptive father, one was the mother’s sister, and one was an aunt. The caregivers’ ages ranged from 23 to 42 years. The majority of them were housewives and had graduated from elementary, junior, and senior high schools.
| Code | Gender | Age | Educational background | Work | Relationship with the child | HIV status | HIV status of the child |
|---|---|---|---|---|---|---|---|
| P1 | F | 36 | Diploma | Private employee | Mother | Positive | Negative |
| P2 | F | 34 | Senior high school | Housewife | Mother | Positive | Negative |
| P3 | F | 42 | Junior high school | Private employee | Mother | Positive | Negative |
| P4 | F | 34 | Elementary school | Self-employed | Mother | Positive | Positive (1) and negative (1) |
| P5 | F | 32 | Senior high school | housewife | Mother | Positive | Negative |
| P6 | M | 39 | Junior high school | Laborer | Adoptive father | Unknown | Positive |
| P7 | F | 38 | Senior high school | Housewife | Mother’s sister | Negative | Positive |
| P8 | F | 32 | Junior high school | Housewife | Mother | Positive | Positive (1) and negative (1) |
| P9 | F | 32 | Elementary school | Housewife | Aunt | Negative | Negative |
| P10 | F | 23 | Elementary school | Housewife | Mother | Positive | Negative |
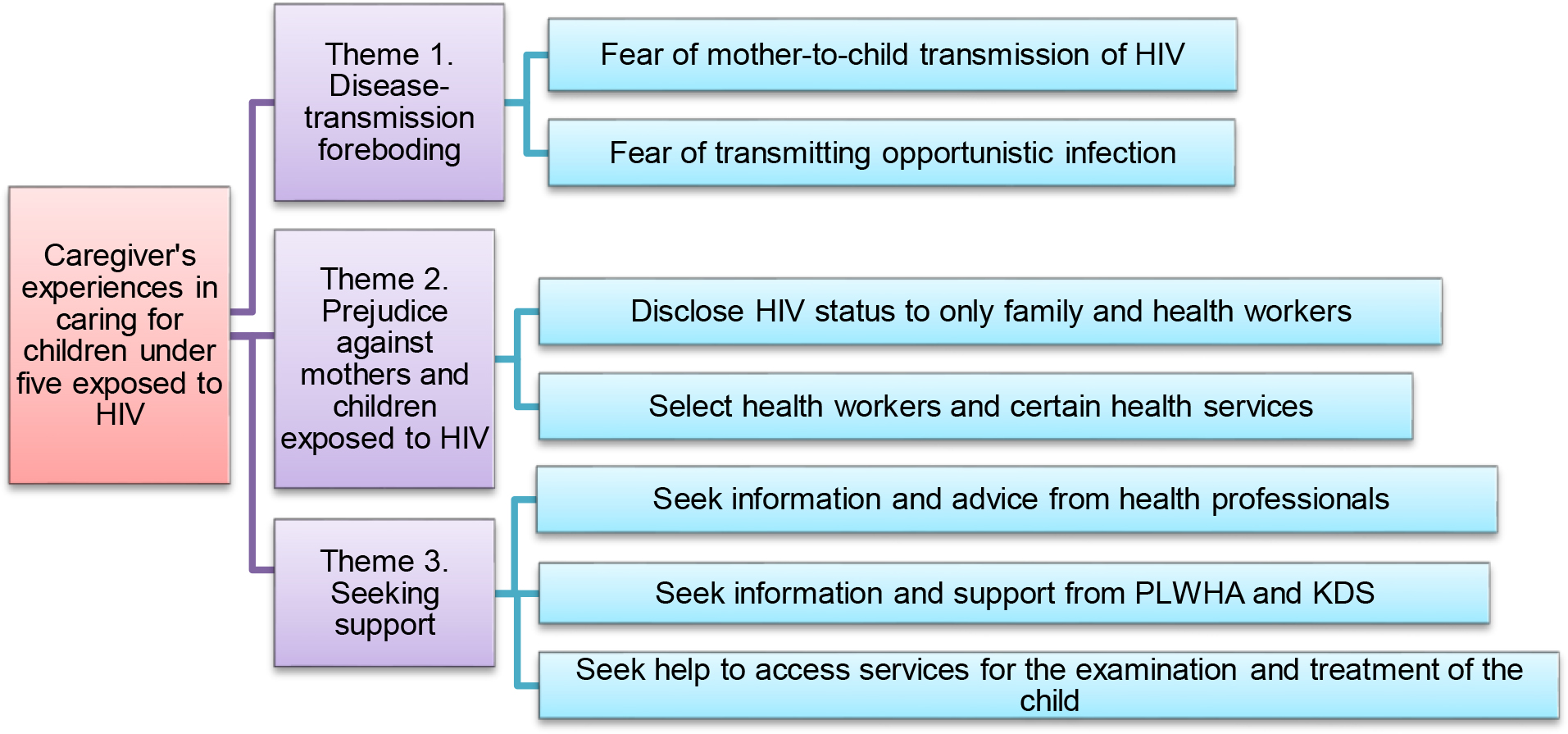
Three themes were generated from the data: 1) disease-transmission foreboding, 2) prejudice against mothers and children exposed to HIV, and 3) seeking support. The coding tree can be seen in Figure 1.
Theme 1. Disease-transmission foreboding
Nine out of ten participants expressed fear of disease transmission. The primary caregiver participants, namely mothers with HIV, were afraid of the risk of HIV transmission from mother to child through breast milk, so they decided not to breastfeed their babies. The participant stated this:
“I was worried when I was pregnant. I was afraid my son would be infected and felt a little scared. I am a bit of a worrier… I am terrified that my son will be the same as his parents.” (P1)
The mother (P1) was worried about the possibility of transferring the virus to her baby. Her worries affected her during pregnancy, childbirth, and after childbirth. She did not want her baby to suffer from the same disease as her mother.
Another mother was worried about how she could give breast milk to her baby.
“When I was pregnant with my third son, I already knew my status, so we consulted with a doctor before the birth… I can give breast milk, but I am afraid. Finally, I decided not to give breast milk, just formula milk.” (P8)
The mother had consulted with health workers before the birth of her third child. Although the mother was allowed to breastfeed, she was afraid that the child would contract HIV due to breastfeeding, so she decided not to breastfeed and used formula milk instead.
Other participants, namely caregivers other than mothers, were concerned about HIV transmission to other family members at home, especially when the child was sick or experiencing opportunistic infections such as diarrhea (P7) and tuberculosis (P6). However, unlike other participants, one participant (P9) stated that they were not afraid of HIV transmission because they already knew how HIV is transmitted and how to prevent transmission.
Theme 2. Prejudice against mothers and children exposed to HIV
The caregivers who participated in the study were either HIV-positive or HIV-negative. The majority of the participants experienced public stigma, particularly from their community or neighborhood. Participants generally kept their HIV status confidential due to the stigma surrounding HIV. They only disclosed their status to spouses, relatives, and health workers involved in their care.
“Some people know, and some do not. I did not tell everyone; only my mother knows… just my mother.” (P4)
The mother (P4) revealed that not all of her family members knew the HIV status of the father, mother, and son.
“The only parent who knows the HIV status is her mother.” (P4)
Stigma concerns also impacted caregivers’ healthcare choices (P3 and P8).
“I do not go to the Posyandu. The problem is, isn’t it better to go to a specialist? There is still a stigma, and I am afraid of being questioned: why isn’t he allowed to receive the polio vaccine? (P3)
The mother (P3) does not take her child to Posyandu, a community-based healthcare center for children under five in Indonesia, for immunizations. Instead, she prefers to take her child to a midwife who knows about her HIV status. The mothers are concerned that questions about their babies’ immunizations will arise due to the stigma in society. Another participant also preferred to visit her usual doctor (P8).
“I am afraid to go to the clinic… I am afraid of discrimination or something. They do not understand… there are still people who stare and judge, so I go to my regular doctor.” (P8)
The mother (P8) prefers to visit the doctor she usually consults because she fears discrimination from other health workers or clinics.
Theme 3. Seeking support
Whether HIV-positive or HIV-negative, the caregivers involved in this study actively sought help in various forms. This assistance included information and advice for child care from health workers, emotional support and information from people living with HIV-AIDS (PLWHA), peer support groups (or called “Kelompok Dukungan Sebaya [KDS]”), and access to health services for examining and treating children. Some of the participants’ expressions are as follows:
“I am going to ask first, when (the child) wants to start eating… instead of looking for info on the internet, it is better for me to ask the health workers, which is for sure.” (P1)
The mother (P1) seeks information and advice from health workers before giving complementary foods to her baby. Other participants sought information about HIV screening services for their babies.
“I do not know how. My son does not have the HIV test yet. There is nothing free. Then they told me to do this and this, finally I got the number contact.” (P2)
The mother (P2) seeks information from friends in KDS, a free HIV screening service for children over one-year-old. However, the examination requires a high cost, as not all Puskesmas have a free HIV testing service program for children (Early Infant Diagnosis / EID).
Other participants, besides mothers (P6), expressed their experiences seeking help from non-governmental organizations (NGOs).
“I am telling you a story. I am having trouble with the pampers. Because, one day, the defecation was eight times. The NGO officer said already, sir, be patient. I will try later. Finally, she came to my house and saw my daughter’s condition.” (P6)
The caregiver (P6) had difficulty meeting the need for diapers when the child had long-lasting diarrhea, so he told the NGO officials about the problem. NGO officials then provided in-person assistance during visits to participants’ homes while examining the child’s condition. Almost all participants, whether maternal or non-maternal caregivers, sought help proactively, demonstrating the need for support in various aspects of caring for children exposed to HIV.
Discussion
This study’s objective was to explore caregivers' experiences caring for children under five exposed to HIV. The study’s findings yielded three themes: disease-transmission foreboding, prejudice against mothers and children exposed to HIV, and seeking support.
Disease-transmission Foreboding
HIV is a contagious disease that can spread through body fluids. Although antiretroviral (ARV) treatment can minimize the risk of mother-to-child HIV transmission, there is still a chance of transmission during pregnancy, childbirth, and breastfeeding. This fact causes many HIV-positive mothers to decide not to breastfeed their babies. The study discovered that most HIV-positive mothers who are caregivers to HIV-exposed children did not breastfeed their infants, even though they had a high CD4 count and an undetectable viral load. In this regard, Ogbo (2016) argued that HIV transmission from mother to child is a significant determinant of suboptimal infant feeding practices, such as non-exclusive breastfeeding, in most African communities with a high prevalence of HIV. Keakabetse et al. (2019) found that mothers’ fear of infecting their babies is one factor that influences infant feeding patterns in children exposed to HIV. Caregivers’ fears about HIV transmission through breastfeeding have led to HIV-exposed children being deprived of breast milk from birth to later stages, unlike children not exposed to HIV.
In contrast, caregivers other than mothers in this study have generally been educated about HIV and know that the disease is not easily transmitted to others. This knowledge makes most caregivers less fearful of HIV transmission in their daily activities. However, caregivers are still concerned about disease and opportunistic infections, such as Tuberculosis. Cowgill et al. (2008) found that many families feared HIV transmission through blood contact, bathroom items, kisses/hugs, and food. Families overcame their fears by educating their children about how HIV is transmitted and setting rules or taking precautions to reduce the risk of HIV transmission in the household. HIV-infected parents are also worried about contracting opportunistic infections from sick children.
Prejudice Against Mothers and Children Exposed to HIV
In society, there is a prejudice against those with HIV, which causes people living with HIV and caregivers to feel anxious if their HIV status is known to others. In this study, the participants expressed their belief that HIV disease is stigmatized in society due to bad deeds and is viewed as a risk for transmission, leading to avoidance from people interacting with people living with HIV (PLWHA). In addition, some mothers participating in the study were concerned that their children would be ostracized if their HIV status was known. Therefore, the participants sought to keep their HIV status private, only disclosing it to healthcare providers and some or all of their family members. This desire for privacy makes caregivers selective in choosing health services for child care. For example, one participant preferred immunization services in midwifery practices rather than public health service facilities like Posyandu because they were concerned that questions would arise about the immunizations obtained by the children.
Related to the results of this study, Muharman et al. (2019) found that older parents move from one place to another to hide their children’s infection status from other family members. This strategy of avoiding stigmatization does not affect health care even if their status is known in health care units. However, there is anxiety that the child will not receive their rights to education, social relationships, and other social support necessary for growth and development whenever the child’s HIV status is known. McHenry et al. (2017), in their research on HIV-infected nannies in Kenya, found that stigma is closely related to the loss of social and economic support but also includes internalized negative feelings about oneself. Participants identified the impact of treatment-related stigma, including non-compliance, the confidentiality of status to children or others, and increased mental health problems.
The results of this study indicate that caregivers’ concerns about stigma and discrimination influence their choice of health services for the children they care for. For this reason, healthcare providers need to consider these caregiver concerns to ensure the fulfillment of the child’s health promotion needs.
Seeking Support
Children exposed to HIV require an early HIV test (EID) to determine their HIV status. Early examination is necessary to ensure that the child receives appropriate treatment. However, this study discovered that several participants encountered obstacles when attempting to obtain EID services. One of the issues is the lack of available tools at health facilities that prevent them from providing EID services. The cost of examinations is also a significant obstacle. The economic status of the participants in this study was a factor, as they all had incomes below the regional minimum wage. These obstacles are similar to those identified in a study by Ernawati et al. (2022), which explored the experience of treating a child with HIV. Themes found in their research include unfamiliarity with HIV disease when treating a child, loss of follow-up related to treatment, limitations for early diagnostic examination, and economic demands in caring for the child.
Children who are exposed to HIV, particularly those who are infected, require intensive treatment due to the repeated infections they experience when their HIV status is unknown. These children need continuous treatment and additional care for any growth and developmental issues they may encounter. In this study, caregivers, other than the mothers, were unaware that the child was infected with HIV. As a result, the child experiences recurrent pain, a deteriorating condition, and delays in receiving antiretroviral (ARV) treatment. In addition, administrative issues, such as the absence of health insurance, contribute to delays in ARV treatment. Caregivers in this study sought assistance accessing healthcare services when the child required hospitalization, managed the child’s health insurance and communicated with healthcare providers while caring for the child at home. Nemathaga et al. (2017), in their study, found that caregivers of children receiving ARV therapy experience financial burdens due to transportation costs needed to comply with follow-up appointments and a lack of funds for necessary food and clothing.
In addition to the child’s condition requiring special attention, caregivers of children exposed to HIV also need specific information for childcare. Caregivers cannot consult anyone freely, only certain people who already know the HIV status of the mother and child being cared for. In this study, caregivers sought information or consulted with health workers in hospitals or health centers who had previous contact with caregivers. They also sought emotional support from PLHIV companions and friends in peer support groups and worked closely with family members when caring for a child at home. Some participants expressed gratitude for receiving help and support from health workers, PLHIV, and peer support group assistants for child care at home.
Our findings align with a study by Sofro and Hidayanti (2019) found that peer support groups can provide social, emotional, self-esteem, and network support, such as intensive communication, strong friendships, and genuine assistance with venture capital, business skills, and medical access. Thus, the combination of peer groups and health professionals plays an essential role in improving the health status of children exposed to HIV through information support, emotional support, and easy access to health services for caregivers and children.
Implications to Nursing Practice and Healthcare Policy
The findings of the study have two significant implications for intervention. Firstly, for informal home-based care for HIV to be a suitable option or alternative to facility-based services in Indonesia, the government needs to implement direct social intervention strategies for families of HIV patients with limited resources. The existing paradigm of facility-based treatment in the country, which primarily consists of medicine refills, counseling, and peer activities, should be modified to include the direct delivery of needs such as psychological assistance to vulnerable households. Secondly, women in Indonesia who are the primary caregivers for HIV patients require social support and intervention programs to assist them. Nursing practices can take an active role in designing intervention programs to improve caregiver well-being and support optimal growth and development in HIV-exposed children under five.
Limitations
Our study, which may be the first to investigate the essential attributes of caregivers living with HIV-exposed children under five in Indonesia, provides a starting point for improving their health status. However, due to stigma, individuals with HIV typically limit interactions and communication with family, PLHIV companions, and peers in the same community, which poses a challenge for researchers to obtain maximum variation.
Conclusion
This study concludes that caregivers of children exposed to HIV generally have disease-transmission foreboding, including HIV transmission from mother to child through breast milk, transmission of HIV to other family members, and opportunistic infectious diseases. In addition, caregivers of children exposed to HIV are concerned about prejudice against mothers and children exposed to HIV, which puts caregivers and children at risk of ill-treatment or discrimination from society. Caregivers of children exposed to HIV require informational assistance, emotional support, and easy access to health services for screening and treatment. Furthermore, most caregivers were female mothers, and the participation of men can indeed be dismissed, despite informal and formal caring seeming to be gendered in most Indonesian contexts. Encouraging the involvement of more males in providing care would be beneficial in gaining their perspectives.