









Background
Cancer is a serious non-communicable disease that is a major problem worldwide, including in Thailand. It is the leading cause of death in Thailand, where as many as 130,000 new patients with cancer are diagnosed yearly (Fongchan et al., 2019). Liver cancer is the third leading cancer in terms of worldwide cancer deaths (Kitiyakara, 2018). Up to 80% of all liver cancer cases worldwide are found in Asia (Vilaichone, 2009). According to data from the World Health Organization (WHO) and the International Agency for Research on Cancer, the likelihood of discovering cancer is 7.9% in males, making it the fifth leading type of cancer (Thai Association for the Study of the Liver, 2015) with three to four times higher prevalence in males than females. In addition, the leading cause of death from cancer in both genders is liver cancer.
Available treatment options for liver cancer include surgical removal of the cancerous tumors, liver transplant, localized destruction of the cancer cells, transarterial chemoembolization (TACE), and palliative care. However, most patients receive the diagnosis after the cancer has metastasized. As a result, the first treatment option for liver cancer is TACE, which increases the survival rate from 10% to 40-50%, covering a period of about 14-20 years (Cabrera & Nelson, 2010).
The side effects of post-TACE cause patients to encounter at least one symptom that impacts them physically, psychologically, emotionally, and socially. Single or multiple symptoms such as abdominal pain and fatigue might occur concurrently. Regardless of the number of symptoms, however, when a single symptom occurs, additional symptoms can follow, and they are interrelated (Cao et al., 2013). If patients experience increased symptom severity or longer symptom duration, various impacts will also increase in severity (Lenz & Pugh, 2018). Suwisith et al. (2008) found that fatigue is the most influential symptom in a person’s daily activities in terms of symptom severity and distress. In addition, Luciani et al. (2008) stated that fatigue is correlated with the activities of daily living, and fatigue in liver cancer patients that have undergone TACE causes more significant disruption to the activities of daily living than before treatment (Cao et al., 2013).
Fatigue is a symptom that persons perceive as physical and psychological abnormalities. The person perceives tiredness, suffering, loss of energy, and weakness. These individual emotional and cognitive perceptions impact the individual’s function and quality of life (National Comprehensive Cancer Network, 2020). Shun et al. (2012) found that fatigue is the leading symptom encountered in patients with hepatocellular carcinoma post-TACE. Fatigue negatively impacts the quality of life (Shun et al., 2008; Sun & Sarna, 2008) and reduces the function status (Khamboon, 2014). In addition, fatigue is the number-one symptom in patients with liver cancer who have undergone TACE and persists even after 4 to 8 weeks post-treatment. Studies have found that fatigue contributes to insomnia, physical weakness, tiredness, and reduces appetite and that all of these symptoms are interrelated, contributing to the premature hospital visits of patients and seriously impacting their quality of life (Li et al., 2015; Nillert et al., 2019; Shun et al., 2012). Thus, fatigue is an influential factor associated with the health status and quality of life of patients post-TACE (Gupta et al., 2007).
Furthermore, fatigue symptoms are the most severe in the 48 hours after treatment (Barsevick et al., 2004; Cao et al., 2013) in 96% of cases. Furthermore, treatment-caused fatigue is also linked to the creation of inflammation such as neopterin, interleukin-1 receptor antagonist, etc. It has been found that fatigue plans for patients with liver cancer treated by TACE are the same plans used for patients with breast cancer that have received chemotherapy (Shun et al., 2005). Studies also have found that the severity of fatigue does not vary among chemotherapy sessions 1-3 (Berger, 1998; Donovan et al., 2004; Greene et al., 1994). However, unrelieved fatigue and reduced functional status may cause patients to withdraw from treatment and negatively impact their lives.
A literature review revealed that preparations for discharge could help patients manage side effects and symptoms that may occur and perform their daily activities by themselves according to their health status (Lan et al., 2015; Salah et al., 2012). It is a process carried out by health professional teams participating in care and continuously meeting the care needs of patients. This process includes transitional care of patients from hospital to home and reciprocal and continuous monitoring to prevent rehospitalization and premature hospital visits while saving treatment expenses. Lan et al. (2015) found that discharge planning can help patients achieve effective self-care and effectively manage side effects in reducing fatigue and depression in liver cancer patients that have received TACE treatment.
The patients during post-TACE have to face unrelieved fatigue and reduced functional status. In addition, the patients only receive routine medical care at the hospital but no follow-up and continuity of care back home. Therefore, this study aimed to determine the effects of a program for comprehensive discharge planning conceptualized by Naylor’s transition care model (Naylor et al., 2004) to help the group mentioned above manage their fatigue and effectively improve their functional status in order to achieve maximum health status.
Naylor et al. (2018) developed the Transitional Care Model (TCM) to improve the care and patient outcomes for people at risk for poor results during the transition period. The TCM is used as a model of care designed to provide comprehensive discharge planning and continuing care, such as patient education, skills training, telephone follow-ups, and home visits (Albert et al., 2015). The comprehensive discharge planning program conceptualized by TCM focuses on nurse-led and interdisciplinary team interventions transferring patients at each stage to facilitate continuous care tailored to the patient’s needs, including the provision of knowledge about illness, treatment, and complication information and fatigue and functional status management. The aim of the study was to investigate the effects of a comprehensive discharge planning program for patients with hepatocellular carcinoma undergoing TACE treatment on their fatigue and functional status post-TACE treatment.
Methods
Study Design
A randomized clinical trial research design was used. The study was conducted from January 2020 to September 2020. The CONSORT (Consolidated Standards of Reporting Trials) checklist (Moher et al., 2010) was used to report the study.
Samples/Participants
The participants in this study were male and female patients with liver cancer aged 18 years and up post-TACE treatment who received arterial chemotherapy at a vascular interventional radiology department, diagnostic radiology, and nuclear medicine unit in a university hospital in Bangkok. The inclusion criteria consisted of patients who could perceive, understand, and communicate in Thai and use a telephone. Exclusion criteria included patients with the end-stage disease (BCLC D) and an ECOG score (Eastern Cooperative Oncology Group) greater than two or post combined TACE and RFA (radiofrequency ablation) treatment or already diagnosed with a psychiatric disorder, such as depression or a cognitive disorder. The researchers used the Thai Mental State Examination (TMSE) to evaluate candidates older than 60. If any candidate scored less than or equal to 23, they might have had cognitive deficiencies that would cause them to be excluded from the study.
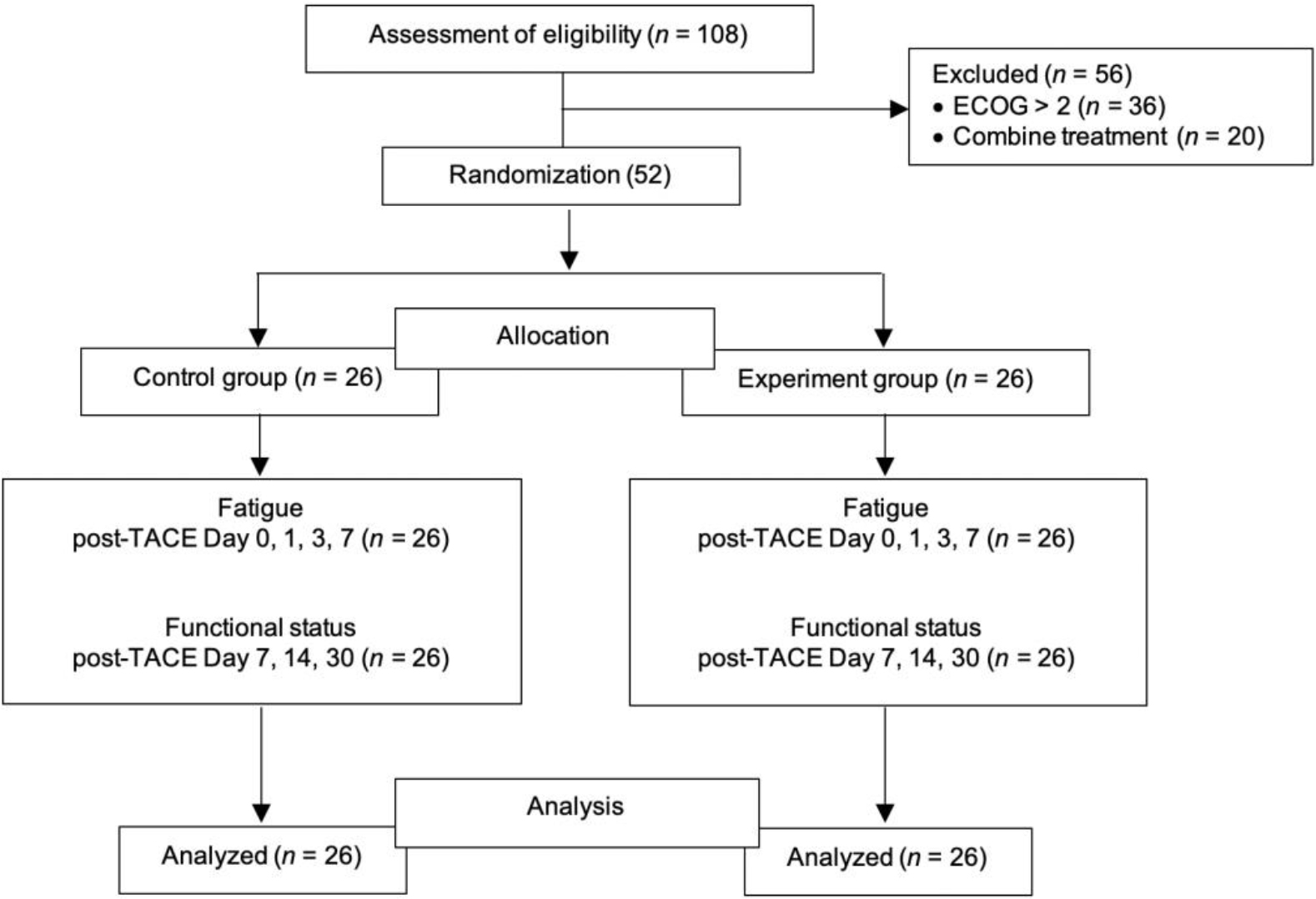
The sample size was calculated using G*Power analysis, with a power of 0.80, α = 0.05, and effect size of 0.86, according to Lan et al. (2015). The results indicated that the study needed 23 samples per group. In order to prevent sample loss, the researchers added an attrition rate of 10%. Therefore, the number of participants was 26 in each group. The researchers randomly assigned samples to the control and experimental groups using simple computerized randomization (Figure 1).
Instruments
Three instruments were used in this study, validated by three clinical experts in cancer care. First, the Demographic and Health related data Questionnaire was used to gather participants’ information such as age, gender, marital status, educational level, religion, occupation, and treatment information, such as disease stage (BCLC stage, and Child-Pugh class), treatment history, number of TACE treatments, co-morbidities, and history of chronic illness medications. Second, the Thai version of the fatigue severity scale, developed by Krupp et al. (1989) and translated into Thai by Sawasdee et al. (2017), was used to measure fatigue severity. It consists of 9 items in the form of Likert scales with values ranging from 1 to 7. A value of 1 indicates no fatigue symptoms/no symptoms/disagreement, while 7 shows a high level of fatigue. Therefore, higher scores mean a higher level of fatigue. The Cronbach's alpha coefficient of the fatigue severity scale was 0.9.
Third, the Thai version of the Enforced Social Dependency Scale (ESDS), developed by Tang and McCorkle (2002) and translated into Thai by Asdornwised et al. (2006), was used to evaluate activities and responsibilities in which patients required assistance from other people due to physical deficiencies. The questionnaire used to assess functional status had possible scores in the range of 10-51. A high score indicated a patient with low functional status. Scores were divided into three levels: scores in the range of 10-23 indicated high functional status. Scores in the range of 24-37 indicated intermediate functional status. Finally, scores in the 38-51 showed low functional status. The reliability of the questionnaire, as determined by using Cronbach's alpha coefficient, equaled 0.89.
Intervention
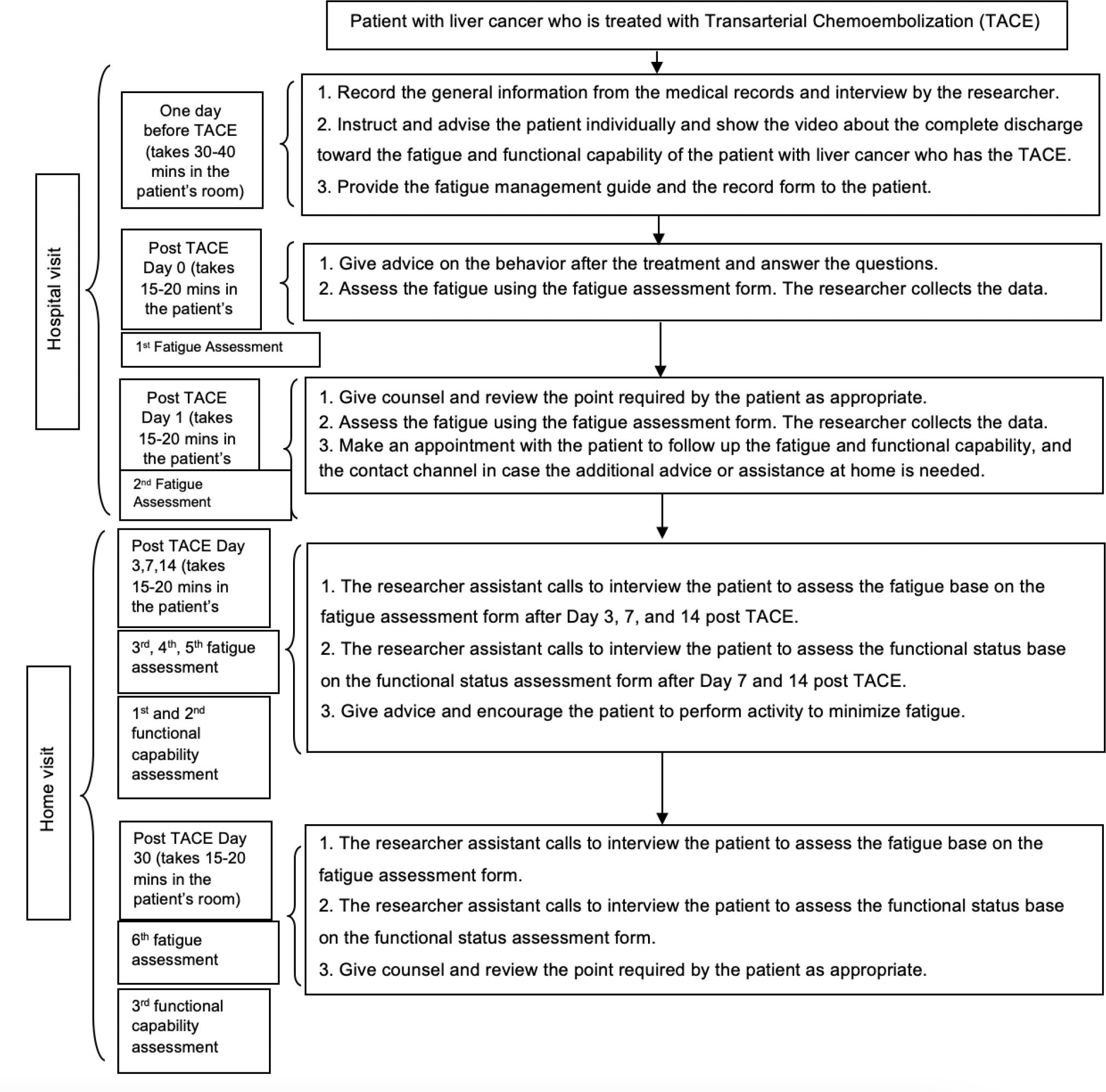
The experimental group received a comprehensive discharge planning program in addition to routine care. The comprehensive discharge planning program was developed based on the Transitional Care Model (Naylor et al., 2018). The healthcare team consisted of a radiologist and registered nurses in radiology who were promoting health outcomes throughout the period from hospital to discharge. The comprehensive discharge planning program consisted of the preparation of patients before discharge from the hospital to home, including the provision of knowledge about the illness, treatment procedures, information about complications and side effects post-treatment, the provision of data about self-care and fatigue management, a handbook, and educational multimedia video clips about fatigue management and functional status management. Three qualified experts, including an interventional radiologist, an oncology nurse, and interventional radiology nurses, validated the program and questionnaire, such as the fatigue and functional status for content validity (CVI = 1). In addition, before the comprehensive discharge planning program was used, it was trialed with ten participants that were representative of the sample group in order to assess the understanding of the content. Overall, the comprehensive discharge planning program intervention consisted of two phases: discharge planning during the hospital visit and four weekly home telephone follow-ups to provide health education, counseling, monitoring, and emotional support tailored to the patient’s needs and using their handbooks. Figure 2 presents the details of the comprehensive discharge planning program intervention.
The control group received routine care (Information about hospitalization, TACE treatment, post-TACE) without access to the comprehensive discharge planning program.
Data Collection
Data were collected using validated questionnaires by the researchers and a research assistant. The research assistant is a nurse with experience in caring for patients with hepatocellular carcinoma undergoing transarterial chemoembolization for at least two years. In addition, the researchers provided training on how to use tools, such as The Fatigue Severity Scale and The Enforced Social Dependency Scale, and the interrater reliability was tested, which has a kappa value of 0.64 and a significance of .05, indicating it is acceptable to collect research data (Pasunon, 2015).
The data collection process in both experimental and control groups is similar (Figure 2). On the day after each sample received TACE (post-TACE Day 0), the researchers met with the patient at the inpatient ward to inquire about post-treatment symptoms and evaluate the person’s fatigue using the fatigue evaluation form. First, the researchers collected data in person (first fatigue evaluation). On Day 1 post-TACE (post-TACE Day 1), the researchers met with each subject in the inpatient ward to inquire about their general symptoms and evaluate their fatigue using the fatigue evaluation form. Then the researchers collected data in person for the second fatigue evaluation. On Days 3, 7, and 14 post-TACE (post-TACE Days 3, 7, and 14) and when the patients were at home, the research assistants interviewed the patients through telephone calls. The patients were evaluated for post-TACE fatigue on Days 3, 7, and 14 and post-TACE functional status on Days 7 and 14 (first and second functional status evaluations). On Day 30 post-TACE, while the patients were at home, the research assistants interviewed the patients through telephone calls. They were evaluated for fatigue (sixth fatigue evaluation) and functional status (third functional status evaluation) and were given consultation as needed by the patients and the doctor’s appointment times.
Data Analysis
SPSS version 25 was used for the data analysis. First, demographic and treatment background data differences were compared using a Chi-squared test and Fisher’s exact test. Next, the differences in the groups’ fatigue and functional status scores were compared using the Wilcoxon signed-rank test. Finally, the Mann-Whitney U test was used to compare the fatigue scores and functional status at different periods between the groups.
Ethical Consideration
The research was conducted after approval from the Institutional Review Board Faculty of Nursing Mahidol University (COA No.IRB-NS2020/549.2402) and approval from the Institutional Review Board Faculty of Medicine, Chulalongkorn University (COA No.334/2020). Each participant signed informed consent prior to data collection. Before signing the informed consent, the researchers first explained the purpose of the study and the confidentiality of the data. The participants could withdraw from the study at any time without penalty. The permissions to use the instruments were granted by the original authors before data collection.
Results
Characteristics of the Participants
A total of 52 participants was divided into 26 participants in the experimental group and 26 in the control group. There were more males (69.2%) than females in both groups. The ages ranged from 37 to 63 years, with most in the range of 60 to 70 years, accounting for 50%. Most participants were Buddhist, were married 69.2%, 28.8% had an elementary level of education, worked as a government official, and had monthly incomes of less than 5,000 baht a month. About half of the participants (51.9%) subscribed to the universal health coverage scheme. Most of them (65.4%) lived in the central part of Thailand and had comorbidity such as diabetes and hypertension (73.1%). Most of the participants were treated by transarterial chemoembolization for the first time (61.5%) with the stage of the disease in Barcelona Clinic Liver Cancer (BCLC) B (86.5%), Child-Pugh (96.2%), and Score 5 (71.2%). The level of the Eastern Cooperative Oncology Group (ECOG) score was mostly at level 0 for 86.5% of the participants. The main side effect of receiving transarterial chemoembolization was fatigue at 9.6%.
Upon comparison of the general characteristics between the experimental and control groups in terms of personal information, such as general information and their medical treatment, it was found that there were no statistically significant differences between the experimental and control groups (Table 1).
| Characteristics of the Participants | Control group | Experimental group | p-value |
|---|---|---|---|
| n (%) | n (%) | ||
| Sex | |||
| Male | 17 (65.4) | 19(73.2) | 0.548C |
| Female | 9 (34.6) | 7 (26.9) | 0.548C |
| Age (years) | 0.856C | ||
| < 60 | 8 (30.8) | 7 (26.9) | |
| 60-70 | 12 (46.1) | 14 (53.9) | |
| > 70 | 6 (23.1) | 5 (19.2) | |
| Religion | |||
| Buddhist | 26 (100) | 26 (100) | |
| Status | 0.631F | ||
| Single | 2 (7.7) | 4 (15.4) | |
| Married | 18 (69.2) | 18 (69.2) | |
| BCLC | 1.000F | ||
| A | 3 (11.6) | 3 (11.6) | |
| B | 23 (88.4) | 22 (84.6) | |
| C | 0 | 1 (3.8) | |
| Child-Pugh | 1.000F | ||
| A | 25 (96.2) | 25 (96.2) | |
| B | 1 (3.8) | 1 (3.8) | |
| ECOG Score | 0.223C | ||
| Score 0 | 21 (80.8) | 24 (92.3) | |
| Score 1 | 5 (19.2) | 2 (7.7) | |
C = p-value from Chi-Square test and F = Fisher’s Exact Test
Fatigue Levels
Table 2 shows the mean and mean ranks for the fatigue scores between the experimental and control groups. The experimental and the control groups on Day 30 had different mean ranks for fatigue that were statistically significant (p = 0.003). The experimental group had a lower mean rank for fatigue than the control group at 1.27±0.58 and 2.50±1.51, respectively. This study found that the comprehensive discharge plan for patients with hepatocellular carcinoma undergoing transarterial chemoembolization can reduce the symptom of fatigue on Day 30 post-TACE at a statistically significant (p <0.05) level.
| Fatigue | Experiment (n = 26) | Control (n = 26) | Mean Rank | Median | IQR | Z | p-value | |||
|---|---|---|---|---|---|---|---|---|---|---|
| Mean | ±SD | Mean | ±SD | Experiment | Control | |||||
| Day 0 | 2.22 | ±1.29 | 2.50 | ±1.51 | 25.37 | 27.63 | 2.00 | 2.00 | 0.546 | 0.585 |
| Day 1 | 2.37 | ±1.40 | 2.49 | ±1.44 | 26.21 | 26.79 | 2.00 | 1.86 | 0.138 | 0.890 |
| Day 3 | 2.60 | ±1.22 | 2.63 | ±1.18 | 26.50 | 26.50 | 2.28 | 1.00 | 0.000 | 1.000 |
| Day 7 | 2.21 | ±1.23 | 2.81 | ±1.36 | 22.75 | 30.25 | 2.11 | 1.75 | 1.790 | 0.073 |
| Day 14 | 1.88 | ±1.04 | 2.27 | ±1.04 | 23.35 | 29.65 | 1.89 | 1.78 | 1.533 | 0.125 |
| Day 30 | 1.27 | ±0.58 | 1.77 | ±0.85 | 20.67 | 32.33 | 1.22 | 0.89 | 2.934 | 0.003* |
p-value from Mann-Whitney U Test,
Functional Status
Table 3 shows the mean rank for the functional status score between the experimental and control groups. The mean rank for functional status at all intervals of patients with hepatocellular carcinoma after undergoing transarterial chemoembolization between the experimental and control groups showed no statistically significant difference (p >0.05). However, there was a difference in the mean rank of functional status in the patients with hepatocellular carcinoma that had undergone transarterial chemoembolization during Days 7-14 between the experimental and control groups that was statistically significant (p = 0.020;). On Day 14, after patients had undergone transarterial chemoembolization, the experimental group had a lower mean rank for functional status from Day 7 than the control group (a lower score means high daily task performance).
| Functional status | Experiment (n = 26) | Control (n = 26) | Mean Rank | Median | IQR | Z | p-value | ||||
|---|---|---|---|---|---|---|---|---|---|---|---|
| Mean | ±SD | Mean | ±SD | Experiment | Control | ||||||
| Time | |||||||||||
| Day 7 | 12.31 | ±1.81 | 13.04 | ±4.25 | 26.56 | 26.44 | 12.00 | 1.75 | 0.028 | 0.977 | |
| Day 14 | 11.62 | ±1.68 | 13.04 | ±4.25 | 23.90 | 29.10 | 12.00 | 1.78 | 1.292 | 0.196 | |
| Day 30 | 11.35 | ±1.44 | 12.69 | ±4.19 | 23.79 | 29.21 | 12.00 | 0.89 | 1.382 | 0.167 | |
| Time Difference | |||||||||||
| Day 7 - Day 14 | 0.69 | ±1.57 | 0.00 | ±0.00 | 29.00 | 24.00 | 0.00 | 0.00 | 2.326 | 0.020* | |
| Day 7 - Day 30 | 0.96 | ±1.75 | 0.35 | ±0.98 | 29.12 | 23.88 | 0.00 | 1.00 | 1.744 | 0.081 | |
p-value from Mann-Whitney U test,
Discussion
Demographic data and health history were tested for differences using the chi-square test. However, the preliminary agreement for the chi-square was not met, so Fisher's test statistics were applied instead. The participants’ personal data and medical histories were not statistically significant between the experimental and control groups (p >0.05).
This study found that the fatigue scores in the experimental and control groups were low and increased on Day 3 post-TACE. This is consistent with Nillert et al. (2019), which found a low fatigue score in patients that received transarterial chemoembolization. The results from this study are also in accordance with Cao et al. (2013) and Shun et al. (2012), which found that fatigue on Day 3 post-TACE increased and gradually decreased during 4-8 weeks after treatment.
This study found that the comprehensive discharge planning program for patients with hepatocellular carcinoma that have undergone transarterial chemoembolization could reduce the symptom of fatigue in the experimental group, which was lower than that of the control group on Day 30 post-TACE at a statistically significant (p <0.05) level (Table 1). The comprehensive discharge planning program includes information about the disease, treatment procedures, complications and side effects after treatment, self-care education, and information about fatigue management. Fatigue management was composed of walking exercise (Ferguson, 2014), muscle exercise (Kim & Seo, 2010), massage (Cawley, 1997), and taking good rest (Tietzel & Lack, 2002). This is consistent with a previous study by Lan et al. (2015), who studied a fatigue management program that resulted in a low level of fatigue. It is also in line with Jaikamsueb (2009) and Srisuksiriphan (2008), who studied walking exercise at home in patients with breast cancer that had received chemotherapy, where it was found that walking exercise at home could reduce fatigue. Also, Tomlinson et al. (2014) found that exercise can reduce fatigue
Moreover, according to the literature review (Koya et al., 2019), it was found that a program that provides knowledge by teaching exercise and follow-up at home can reduce the symptom of fatigue and can also reduce anxiety as well as prepare patients to cope with side effects. When the patient is discharged from the hospital and receives follow-up by the nurse specialist, they have a better quality of life, and their return to the hospital before the appointment date is reduced (Salah et al., 2012).
This study also found that the comprehensive discharge program helped increase the functional status of patients with hepatocellular carcinoma that had undergone transarterial chemoembolization. There was a difference in the mean rank of functional status in patients with hepatocellular carcinoma undergoing transarterial chemoembolization during Days 7-14 between the experimental and control groups that was statistically significant (p = 0.020). On Day 14, after the patients had undergone transarterial chemoembolization, the experimental group had high functional status (a lower mean rank for functional status) from Day 7 than the control group.
The patients are more capable of performing daily activities as well as living in society. This is in accordance with Cheville et al. (2013) and Tsianakas et al. (2017) found that a home-based walking exercise program reduced fatigue and increased the ability to perform daily activities, quality of life, and the patient’s self-care.
Implications of the Study
This comprehensive discharge program provides recommendations and practices for when the patient returns home, fatigue and clinical risk management, follow-ups as appointed, and home follow-ups. The patients that have received TACE should be encouraged to engage in self-care education and symptom follow-up when returning home. This is in line with Luciani et al. (2008) found that discharge planning before returning home can reduce the symptom of fatigue and depression in patients with hepatocellular carcinoma that have undergone transarterial chemoembolization at a statistically significant level. The discharge planning program comprises the patient's preparation for admission and preparation when being discharged from the hospital and following up with a specialized health team. As Gupta et al. (2007) stated, the patients’ follow-up could improve their quality of life and satisfaction and increase self-care ability.
In addition, this comprehensive discharge planning program effectively reduces fatigue symptoms and enhances the functional status of patients with hepatocellular carcinoma undergoing transarterial chemoembolization. Therefore, the comprehensive discharge planning program developed in this study can be used by nurses and multidisciplinary teams in order to achieve the effectiveness of nursing care for patients nationally and internationally.
Limitations of the Study
Patients might receive knowledge and advice on how to behave from a doctor or radiologist more and less differently; however, each patient receives equal time for advice. It might affect the patients' practice during staying at home.
Conclusion
The comprehensive discharge planning program was found to be effective in reducing fatigue and improving functional status. By creating a discharge plan for patients before returning home, the patients can be encouraged to take care of themselves effectively and manage their complications. In addition, this comprehensive discharge planning prepares patients for treatment, for being ready when they are discharged from the hospital, and for continued monitoring with a specialized healthcare team. A comprehensive discharge planning program is still being used in hospitals with a multidisciplinary collaboration to reduce fatigue and improve self-care after TACE treatment. Thus, the researchers recommend that nurses use the discharge planning program alongside planning performance improvements involving multiple disciplines to produce desirable outcomes for patients and their families.