










Background
Mental health literacy (MHL) denotes a construct of the health literacy domain that underlines an individual’s knowledge of mental wellness (Kutcher et al., 2016; Milin et al., 2016). People and communities require MHL to identify illnesses and maintain health by knowing where to access health information. The knowledge of mental health disorders encompasses cognitive and social competence to promote sound mental health. Individuals and communities should understand policies, treatments, and self-management capabilities for mental disorders through MHL (Furnham & Swami, 2018). The Kingdom of Saudi Arabia (KSA) deals with a wide incidence of mental disorders. According to the first Saudi National Health and Stress Survey by Al-Twaijri et al. (2019), 2 in 5 Saudi youth aged 15–24 years develop mental health issues at a particular stage in their lives, yet only 5% seek out treatment or support.
World Health Organization (2019) reported that mental health disorders such as depression, bipolar disorders, schizophrenia, dementia, and psychosis affect more than 25% of the global population, including university students. KSA registers a high prevalence rate, particularly in institutions of higher learning, as per Al-Twaijri et al. (2019). The government commissioned the King Abdullah International Medical Research Centre to develop a policy framework that tackles mental disorders and discrepancies in literacy and treatment of 48% of the population (Almutairi, 2015). University academic staff participate in the promotion of MHL, as they are in direct contact with students who are susceptible to such challenges and often play the dual role of academic advisors and counselors.
Academic advisors in the educational environment are the potential gatekeepers of students’ mental health. They can be the first in line to detect indicators of mental illnesses in students and can refer them to appropriate mental health services (Gulliver et al., 2019). Academic faculty staff plays the dual role of instructors and academic advisors. Thus, academic staff should be trained in mental health so that they are suitably placed to provide professional direction for university students dealing with mental disorders like depression, bipolar disorder, and any mental health issue that may attract stigma. World Health Organization (2019) has acknowledged the existence of mental health disorders in KSA and the need for high-priority care and research. However, the mental health literacy of academic advisors managing learners with mental health problems in KSA remains unclear.
According to Buchanan (2012), only a few college students seek medical health interventions when they develop mental health problems despite the availability of university counseling services. KSA struggles with a lack of evidence-based support in the educational environment. Gulliver et al. (2019) identify causes such as inadequate public awareness and academic staff lacking the necessary training and resources to deal with students with mental health problems.
Academic advisors should be aware of MHL when dealing with students. However, despite the importance of this issue, only a few studies have been conducted in this field. These studies have found that many academic staff members have difficulty delivering professional assistance to students due to an insufficient level of MHL (Frauenholtz et al., 2017). Problematic areas include symptom identification, unavailability of mental health services, psychotropic medication, and stigmatization of the learners (Abid, 2018). Notably, none of the studies reviewed by the researcher was conducted within the context of KSA.
Svensson and Hansson (2016) probed the connection between MHL, the experience of mental illnesses, and stigma in 1027 Swedish staff members. They found that at least 50% of MHL in staff influences the students’ depression and reduces negative attitudes and social distance. However, findings relating to a developed economy such as Sweden cannot be applied to a developing country such as KSA. Furthermore, the researcher is aware of a lack of awareness among academic advisors on handling students with mental health problems. Therefore, this study assesses the academic advisors’ MHL and their experiences with students facing mental health problems at King Abdulaziz University (KAU).
This research will contribute to understanding MHL among academic advisors at KAU in KSA. It will help bridge the gap that complicates the help-seeking behaviors of learners struggling with mental health difficulties. Further, this research will reveal the effort made by educational institutions and the government to equip teachers with the expertise and competencies to minimize mental health problems among students at KAU. Additionally, the findings should stimulate a discourse on the mental health issues faced by learners in different academic institutions.
Methods
Study Design
A descriptive cross-sectional study design was implemented among academic advisors from the medical campus at a governmental University in Jeddah, Saudi Arabia. The medical campus includes a number of health sciences, including Nursing, Medicine, Dentistry, Nutrition, Laboratory studies, Pharmacy, etc.
Sample/Participants
The sample size was calculated using Raosoft software (Raosoft, 2004) with a confidence interval of 5% and confidence level of 95% on the basis of the total number of health sciences academic staff members from each faculty on the medical campus at a governmental University in Jeddah, Saudi Arabia. The calculated sample size was 133 academic advisors from different health science backgrounds. Convenience sampling was used to collect the data. The inclusion criteria were academic advisors from different health science backgrounds with more than one year of experience and direct contact with the students. The rationale for including faculty members from various health science backgrounds is the current trend and emphasis on the importance of Interprofessional Education (IPE) in health sciences, research, and patient safety (Yune et al., 2020). IPE refers to the collaborative practice among healthcare professionals, including nurses, physicians, pharmacists, and dentists, with other healthcare professionals to perform their assigned tasks and enhance their competencies (World Health Organization, 2010). Collaborative practice and communication among those from different health science backgrounds are essential as healthcare students are likely to be taught and interact with faculty members from other health specialties. Therefore, the inclusion of faculty members of different health science backgrounds is expected to lead to the development of richer views and perspectives of academic advisors from other health science backgrounds (Aston et al., 2012).
Instruments
The data were collected through a three-part electronic questionnaire created using Google Forms and shared through social media (Email and WhatsApp messenger) from November 2020 to February 2021. The authors of this study developed the first and second parts of the questionnaire. The questionnaire was distributed in English and did not require translation into Arabic, as health sciences in Saudi Arabia are taught in English. Therefore, faculty academic advisors are fluent in the English language.
Part one of the questionnaire assessed the demographic and professional attributes of the study participants. It comprised eight questions related to age, nationality, teaching role, specialty/department, teaching/supervising level, and years of teaching or supervising at the university.
Part two of the questionnaire assessed the participants’ experience when they assisted learners with mental health difficulties. This part comprised five closed-ended, Yes/No questions. Participants answered the following questions: Have you ever taught a student with a mental health problem?; Have you ever initiated a conversation or discussed with a student about their mental health problem(s)?; Have you been approached or confided in by a student who faced a mental health problem?; Has a student ever told you that they have suicidal thoughts?; Have you felt sufficiently informed to respond appropriately to a learner with a mental health crisis?
Part three of the questionnaire was the Mental Health Literacy Scale (MHLS) adopted from OConnor and Casey (2015). Permission was sought from the authors to adopt the questionnaire for assessing study participants’ knowledge of various aspects of dealing with mental health problems. The MHLS contains 35 items (with five reverse questions) measuring the three domains of MHL. The first domain measures the ability to identify mental disorders (Items 1–8). The second domain concerns itself with the knowledge of various risk factors and causes, professional help, self-treatment, and sources of information seeking (Items 9–19) (with items 10, 12, and 15 in this domain being reverse statements). The final domain speaks of negative attitudes (Items 20–28) and positive attitudes (Items 29–35) concerning mental illness (with items 20–28 in this domain being reverse statements). The MHLS requires respondents to rate the items on a 4-point scale, ranging from 1= “Very unlikely/unhelpful” to 4= “Very likely/helpful”, or a 5-point scale, ranging from 1= “Strongly disagree/definitely unwilling” to 5= “Strongly agree/definitely willing.” (OConnor & Casey, 2015). The first 15 items were scored on a 1–4 scale, with items 10, 12, and 15 being scored in reverse. Items 16–35 were scored on a 1–5 scale, with items 20–28 being scored in reverse. The total score was generated by summing all items (Max score=160; Min score=35). These scores can range from 35 to 160, with the following levels of classification: 35–77: low; 78–118: moderate; 119–160: high.
The tool was examined for its face and content validity by an expert advisory group, which consisted of three academic experts from the Psychiatric and Mental health nursing field. Further, the reliability of the instrument was tested in this study on November 10, 2020, and Cronbach’s Alpha coefficient α was 0.782 for the 35 items of the MHLS. The reliability of the three domains also showed an acceptable level of Cronbach’s alpha values. The overall reliability results indicated that the questionnaire’s reliability was of good internal consistency. Moreover, before starting the actual study, the primary investigator selected approximately 10% (16) of the academic advisors that met the selection criteria for the study to participate in a pilot study. The pilot study was conducted after receiving ethical approval to oversee the research study from the ethical board at the study institution. The pilot study ensured that the tool was feasible, understandable, clear, free from jargon, and easy to understand; no specific modifications were needed to be introduced to the study tool following the pilot study. Hence, the primary researcher decided to include pilot study participants within the actual research to reach the target sample size (Thabane et al., 2010).
Data Analysis
Data were studied using Statistical Packages for Social Sciences (SPSS) version 26.0. Descriptive statistics (mean, standard deviation, frequencies, and percentages) were sought to illustrate the quantitative and categorical variables. Cronbach’s alpha was used to assess the internal consistency of items of MHLS. Student’s t-test for independent samples and one-way analysis of variance followed by Tukey’s test were used to match the mean scores of MHLS versus the demographic and professional attributes of academic advisors. A p-value of ≤ 0.05 reported the statistical significance of the outcomes.
Ethical Considerations
Ethical approval to conduct this study was sought from the Nursing Research Ethics Committee (NREC) at the Faculty of Nursing at King Abdulaziz University (NREC Serial No: Ref No 1M. 22). Furtherer, written informed consent from the study participants was obtained. Confidentiality of individual responses was promised in a clear statement on the cover page, and complete information on the study was provided to the participants. Participants’ anonymity was retained by asking them to avoid putting their names or any identifying personal data on the questionnaire. In addition, the participants were briefed on their right to withdraw from the study at their convenience. The data collected were stored safely, with only the research team that has access to it.
Results
The demographic and professional attributes of the academic advisors are presented in Table 1. Approximately two-thirds (67%) fell in the younger age group (≤40 years), nearly all were female (83%), and predominantly from Saudi (74%). The most frequently mentioned academic position was assistant professor (39 %), followed by lecturer (26%). Further, the participants’ teaching roles included lecturing (81.2%), research supervision (45.1%), and clinical supervision (34.6%). The most commonly mentioned departments were medicine (36%), nursing (15%), and dentistry (14 %). Moreover, most respondents were teaching/supervising bachelor-level students (83.5%), with the remaining respondents teaching/supervising master’s level students (37.6%) and PhD level students (6.8%).
| Demographic and professional characteristics | n | % |
|---|---|---|
| Age group | ||
| ≤40 years | 89 | (67%) |
| >40 years | 44 | (33%) |
| Gender | ||
| Male | 22 | (17%) |
| Female | 111 | (83%) |
| Nationality | ||
| Saudi | 98 | (74%) |
| Non-Saudi | 35 | (26%) |
| Academic categories | ||
| Clinical instructor | 21 | (16%) |
| Lecturer | 35 | (26%) |
| Assistant professor | 52 | (39%) |
| Associate professor | 11 | (8%) |
| Professor | 14 | (11%) |
| Teaching role * | ||
| Lecturing | 108 | (81.2%) |
| Research supervision | 60 | (45.1%) |
| Clinical supervisor | 46 | (34.6%) |
| Department | ||
| Medicine | 48 | (36%) |
| Dentistry | 19 | (14%) |
| Pharmacy | 14 | (11%) |
| Nursing | 20 | (15%) |
| Laboratory sciences | 15 | (11%) |
| Others | 17 | (13%) |
| Teaching/supervising level * | ||
| Baccalaureate level students | 111 | (83.5%) |
| Master level students | 50 | (37.6%) |
| PhD level students | 09 | (6.8%) |
| Years of teaching experience | ||
| ≤10 years | 74 | (56%) |
| >10 years | 59 | (44%) |
Table 2 describes the statements of the recognition domain of the MHLS. The highest weighted mean score obtained (3.56 ± 0.59) implies agreement with the statement, “To what extent do you think it is likely that the diagnosis of bipolar disorder includes experiencing periods of elevated (i.e., high) and depressed (i.e., low) mood.” Conversely, the lowest weighted mean score was 3.22 ± 0.58, which indicates that academic advisors are likely to agree with the statement, “To what extent do you think it is likely that the diagnosis of agoraphobia includes anxiety about situations where escape may be difficult or embarrassing.”
| Statements of recognition domain of Mental Health Literacy Scale | Mean ± SD | Overall Response |
|---|---|---|
| 1- If someone became extremely nervous or anxious in one or more situations with other people (e.g., a party) or performance situations (e.g., presenting at a meeting) in which they were afraid of being evaluated by others and that they would act in a way that was humiliating or feel embarrassed | 3.27 ± 0.64 | Likely |
| 2- If someone experienced excessive worry about a number of events or activities where this level of concern was not warranted, had difficulty controlling this worry, and had physical symptoms | 3.34 ± 0.61 | Likely |
| 3- If someone experienced a low mood for two or more weeks, had a loss of pleasure or interest in their normal activities, and experienced changes in their appetite and sleep, then to what extent do you think it is likely they have Major Depressive Disorder | 3.37 ± 0.67 | Likely |
| 4- To what extent do you think it is likely that Personality Disorders are a category of mental illness | 3.26 ± 0.71 | Likely |
| 5- To what extent do you think it is likely that (Persistent Depressive Disorder) is a disorder | 3.55 ± 0.66 | Very likely |
| 6- To what extent do you think it is likely that the diagnosis of Agoraphobia includes anxiety about situations where escape may be difficult or embarrassing. | 3.22 ± 0.58 | Likely |
| 7- To what extent do you think it is likely that the diagnosis of bipolar disorder includes experiencing periods of elevated (i.e., high) and periods of depressed (i.e., low) mood | 3.56 ± 0.59 | Very likely |
| 8- To what extent do you think it is likely that the diagnosis of Substance Abuse Disorder includes physical and psychological tolerance of the drug | 3.30 ± 0.66 | Likely |
| Total Mean ± SD | 26.9 ± 3.25 | |
| Cronbach’s alpha: 0.785 (95% C.I: 0.726 to 0.836) |
Table 3 indicates that the highest weighted mean score for the knowledge domain of the MHLS was 4.15 ± 0.88, which shows that academic advisors agree with the statement, “I am confident that I know where to seek information about mental illness.” Conversely, the lowest weighted mean score was 2.02 ± 0.73 in response to the statement, “To what extent do you think it would be helpful for someone to avoid all activities or situations that made them feel anxious if they were having difficulties managing their emotions.”
| Statements of knowledge of risk factors and causes, professional help, self-treatment, and knowledge of sources of information seeking domain of Mental Health Literacy Scale | Mean ± SD | Overall Response |
|---|---|---|
| 9- To what extent do you think it is likely that in Saudi Arabia women are MORE likely to experience a mental illness of any kind compared to men | 3.10 ± 0.76 | Likely |
| 10- To what extent do you think it is likely that in Saudi Arabia men are MORE likely to experience anxiety disorder compared to women | 2.22 ± 0.72 | Likely |
| 11- To what extent do you think it would be helpful for someone to improve their quality of sleep if they were having difficulties managing their emotions | 3.37 ± 0.62 | Helpful |
| 12- To what extent do you think it would be helpful for someone to avoid all activities or situations that made them feel anxious if they were having difficulties managing their emotions | 2.02 ± 0.73 | Helpful |
| 13- To what extent do you think it is likely that Cognitive Behaviour Therapy (CBT) is a therapy based on challenging negative thoughts and increasing helpful behaviors | 3.38 ± 0.59 | Likely |
| 14- To what extent do you think it is likely that the following is a condition that would allow a mental health problem to break confidentiality; If you are at immediate risk of harm to yourself or other | 3.47 ± 0.59 | Very likely |
| 15- To what extent do you think it is likely that the following is a condition that would allow a mental health problem to break confidentiality; if your problem is not life-threatening and they want to assist others to better support you | 2.26 ± 0.82 | Likely |
| 16- I am confident that I know where to seek information about mental illness | 4.15 ± 0.88 | Agree |
| 17- I am confident using the computer or telephone to seek information about mental illness | 3.96 ± 1.05 | Strongly agree |
| 18- I am confident attending face-to-face appointments to seek information about mental illness [e.g., seeing the General Practitioner (GP)] | 3.86 ± 0.99 | Agree |
| 19- I am confident I have access to resources (e.g., GP, internet, friends) that I can use to seek information about mental illness | 3.95 ± 0.96 | Agree |
| Total Mean ± SD | 35.73 ± 4.00 | |
| Cronbach’s alpha: 0.606 (95% CI: 0.499 to 0.699) |
The main scores and standard deviation of the academic advisors’ responses to the attitude domain in the MHLS Scale are displayed in Table 4. The highest weighted mean score was 4.17 ± 1.06, which shows academic advisors strongly disagreed with the statement, “A mental illness is not a real medical illness.” However, the lowest weighted mean was 2.53± 1.15 in response to the question, “How willing would you be to vote for a politician if you knew they had suffered a mental illness?” The total main score for the level of the attitudinal domain was 56.5 ±11.42.
| Statements of attitude domain of Mental Health Literacy Scale | Mean ± SD | Overall Response |
|---|---|---|
| 20-People with a mental illness could snap out if they wanted | 2.78 ± 1.01 | Agree |
| 21-A mental illness is a sign of personal weakness | 3.84 ± 1.12 | Strongly disagree |
| 22-A mental illness is not a real medical illness | 4.17 ± 1.06 | Strongly disagree |
| 23-People with a mental illness are dangerous | 3.43 ± 1.08 | Neutral |
| 24-It is best to avoid people with a mental illness so that you don't develop this problem | 4.05 ± 0.97 | Strongly disagree |
| 25-If I had a mental illness, I would not tell anyone | 3.33 ± 1.17 | Neutral |
| 26-Seeing a mental health professional means you are not strong enough to manage your own difficulties | 4.01 ± 1.10 | Strongly disagree |
| 27-If I had a mental illness, I would not seek help from a mental health professional | 4.06 ± 1.03 | Strongly disagree |
| 28-I believe treatment for a mental illness, provided by a mental health professional, would not be effective | 4.16 ± 1.01 | Strongly disagree |
| 29-How willing would you be to move next door to someone with a mental illness? | 3.45 ± 1.03 | Willing |
| 30-How willing would you be to spend an evening socializing with someone with a mental illness? | 3.59 ± 0.95 | Willing |
| 31-How willing would you be to make friends with someone with a mental illness? | 3.54 ± 0.89 | Willing |
| 32-How willing would you be to have someone with a mental illness start working closely with you on a job? | 3.49 ± 1.04 | Willing |
| 33-How willing would you be to have someone with a mental illness marry into your family? | 2.77 ± 1.09 | Neutral |
| 34-How willing would you be to vote for a politician if you knew they had suffered a mental illness? | 2.53 ± 1.18 | Definitely Unwilling |
| 35-How willing would you be to employ someone if you knew that they had a mental illness? | 3.20 ± 1.04 | Willing |
| Total Mean ± SD | 56.5 ± 11.42 | |
| Cronbach’s alpha: 0.824 (95% CI: 0.777 to 0.864) |
Table 5 displays the comparison of the study subject’s mean mental health literacy scores for their demographic and professional traits. Mental Health Literacy levels among our study subjects were found to be high (53.4%) and moderate (46.6%). The mean (SD) of the MHL scale of all subjects was 119.0 (11.71).
| Characteristics | Mean (SD) | t/F-value | p-value |
|---|---|---|---|
| Age groups (in years) | |||
| ≤ 40 | 117.73 (12.3) | -1.941 | 0.055 |
| >40 | 121.59 (9.9) | ||
| Gender | |||
| Male | 117.81 (10.6) | -0.520 | 0.604 |
| Female | 119.24 (11.9) | ||
| Nationality | |||
| Saudi | 118.43 (12.0) | -0.953 | 0.342 |
| Non-Saudi | 120.63 (10.7) | ||
| Experience (in years) | |||
| ≤ 10 years | 118.55 (11.4) | -0.953 | 0.342 |
| >10 years | 119.58 (12.2) | ||
| Teaching role: Lecturer | |||
| Yes | 120.12 (11.8) | 2.315 | 0.022* |
| No | 114.20 (10.3) | ||
| Teaching role: Research supervision | |||
| Yes | 121.15 (10.4) | 1.932 | 0.056 |
| No | 117.25 (12.5) | ||
| Teaching role: Clinical supervisor | |||
| Yes | 115.80 (11.1) | -2.331 | 0.021* |
| No | 120.70 (11.7) | ||
| Academic position | |||
| Clinical instructor | 111.09 (9.9) | 6.506 | <0.001* |
| Lecturer | 116.88 (10.2) | ||
| Assistant professor | 124.32 (10.9) | ||
| Associate professor | 119.36 (12.4) | ||
| Professor | 116.14 (12.3) | ||
| Working department | |||
| Medical | 116.04 (11.1) | 2.181 | 0.060 |
| Dentistry | 116.95 (12.3) | ||
| Pharmacy | 117.93 (14.4) | ||
| Nursing | 121.40 (11.8) | ||
| Laboratory sciences | 125.60 (8.9) | ||
| Others | 121.94 (10.2) |
Comparing mean values of the MHL total score in relation to the demographic and professional characteristics showed a significant difference in the final mean scores with regard to the professional attributes (Teaching role: lecturer, clinical supervisor, and academic position). The mean mental health literacy score was statistically significantly higher in academic advisors who had a teaching role as lecturer when compared with those who did not have a teaching role as a lecturer (t = 2.315; p = 0.022). Also, the mean mental health literacy score was statistically significantly higher in academic advisors who did not have a teaching role as a clinical supervisor compared to those who had a teaching role as a clinical supervisor (t = -2.331; p = 0.021). In addition, the mean mental health literacy scores were statistically significantly higher in academic advisors who had academic positions of lecturer, assistant professor, fellow professor, and professor when compared with those academic supervisors who were clinical instructors (F = 6.506; p <0.001).
The pairwise comparison of mean scores indicated no difference among the pairs of academic advisors who were lecturer, assistant professor, associate professor, and professor. In contrast, the mean mental health literacy scores were not statistically significantly different compared to the other characteristics (age groups, nationality, participants’ gender, working experience, teaching role: research supervision, and department).
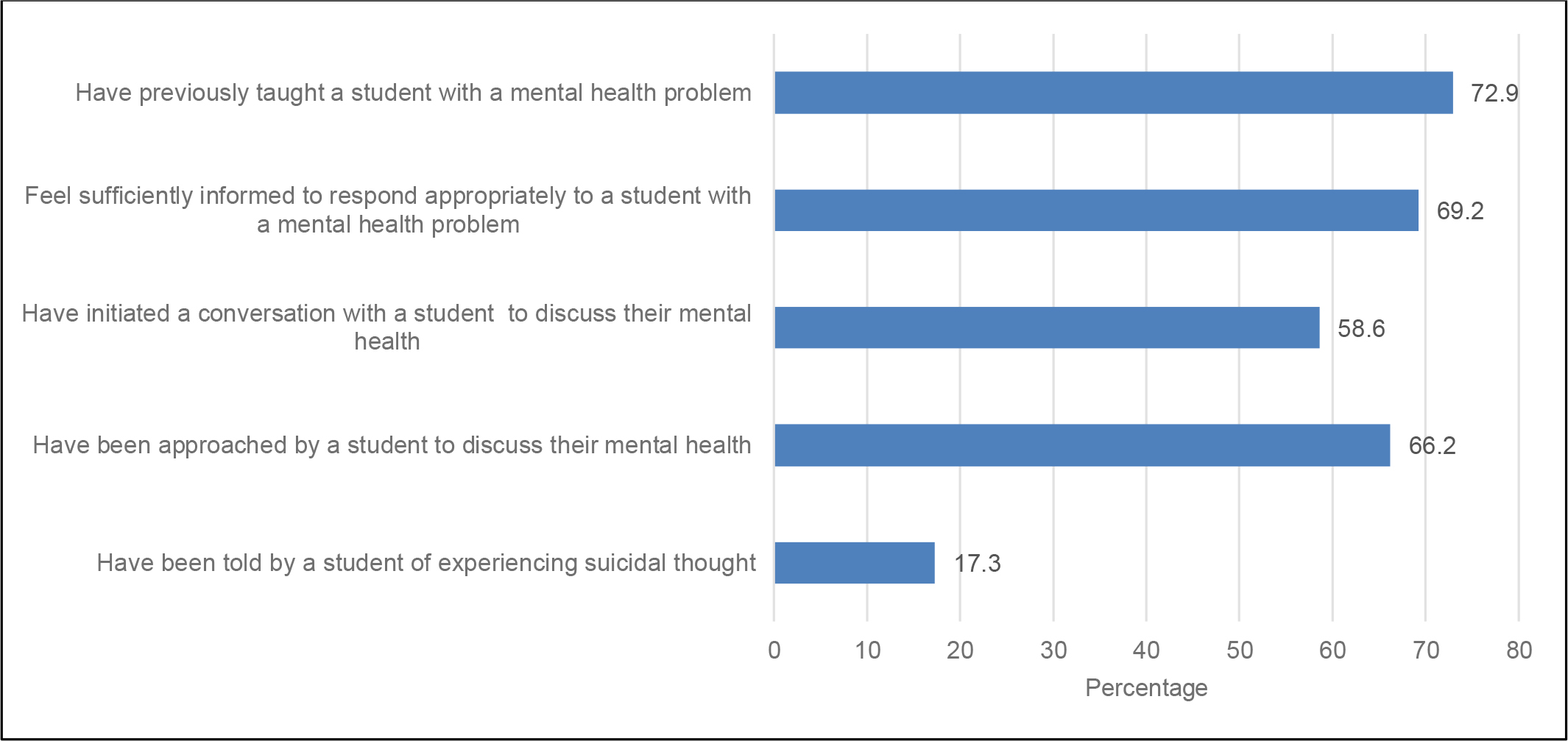
Figure 1 indicates the academic advisors` experience dealing with learners’ mental health challenges. It was found that most academic advisors “have previously taught a student with a mental health problem” (72.9%). In addition, the majority “feel sufficiently informed to respond appropriately to a student with a mental health problem” (69.2%), “have been approached by a student to discuss their mental health” (66.2%), and “have initiated a conversation with a student to discuss their mental health” (58.6). Only 17.3% of advisors “have been told by a student of experiencing suicidal thoughts.”
Discussion
The study aimed to assess academic advisors’ mental health literacy and their experiences of dealing with learners facing mental health problems. However, no statistically significant relationship was found between demographic characteristics and mental health literacy. This could be because the academic advisors that participated in this study had more than ten years of work experience in the role of an academic advisor. Further, most participants were female. This, coupled with their years of experience and opportunities to interact with students at an individual or group level, may have helped shape their mental health literacy. This finding differs from the results of Khan et al. (2018) that academic staff with 1–5 years of work experience had higher MHL than staff with more than five years of experience in the faculty. This is because the younger staff have more current knowledge about things around them. Regarding gender, the findings are also contrary to the outcomes of Parikh et al. (2016) that female teachers had lower knowledge levels and negative attitudes and beliefs towards students’ mental ailments than their male counterparts. Conversely, in a study undertaken in Nigeria, Aluh et al. (2018) reported that females showed higher mental health literacy than males.
Regarding academic advisors’ experiences when dealing with students’ mental health problems, this study revealed that advisors’ years of experience in handling students’ mental health problems shaped their MHL. It was revealed that the most commonly mentioned experience when dealing with students’ mental health problems was having taught an undergraduate with a mental health difficulty, followed by feeling satisfactorily knowledgeable to respond suitably to a similar learner and having been contacted or confided in by a learner who faced such difficulties. From the researcher’s perspective, the academic advisors’ interactions with the learners during lessons and reading up on information about their mental health conditions allowed them to offer guidance to the learners. This finding is supported by Gulliver et al. (2019) and Farrer et al. (2015) found that university staff obtained high MHL scores because they sought sufficient information from students with mental health problems. Knowledge creates a personal experience with students’ mental health struggles, which then shapes the assistance offered and helps overcome negative attitudes or stigma associated with the conditions. Lo et al. (2018) found that mental health literacy reduces the social distance between academic staff and students with mental health issues, which subsequently builds help-seeking behaviors.
Nevertheless, the results were inconsistent with those obtained by Aluh et al. (2018), who found that study participants lacked foundational knowledge about depression. Subsequently, the advisors could not interpret or label the mental health problems or identify the key symptoms affecting the students. The low level of MHL among academic advisors exposes students to stigma (Gulliver et al., 2019). The academic advisors cannot safeguard the learners from stigmatizing attitudes without proper experience and knowledge about depression or the mental health issue affecting them.
The current study also analyzed how MHL varies with the professional characteristics of academic advisors. Lecturers were found to possess a higher level of MHL than professors, associate professors, or assistant professors, but there were statically significant differences between them. The lecture’s duration and level of interaction with the students allow them to detect any mental health problems, offer advice, and follow up on students with mental health problems. The findings are consistent with Khan et al. (2018) noted that Pakistani academic staff had varying knowledge of mental issues and that they moderated the beliefs of the learners about their mental health conditions. Therefore, students are more prone to facing negative attitudes when the staff lacks a basic understanding of their depression, stress, fears, or worries instigated by the academic environment or personal struggles. Students cannot receive proper guidance when some academic advisors lack sufficient knowledge about their mental health problems. The researcher refers to the results related to the high level of knowledge and experience of academic advisors gained through continuous contact with students as well as an annual meeting about the role and responsibilities of the academic advisor during which students can discuss any problems they are facing and ways of handling them. Khan et al. (2018) and Farrer et al. (2015) suggest that recovery from mental health problems depends on the knowledge and experience of the advisors with whom the students share their struggles. The learners consult, seek support, and get referrals from academic advisors who understand their mental health problems.
This study’s findings also indicate the value of a teacher in fostering MHL and providing mental health aid to learners. Lecturing appears to be more significantly related to increased MHL scores than clinical supervision or research supervisor roles. This could be because lecturers have more direct contact with students than research and clinical supervisors. Lo et al. (2018) state that when they assessed the interventions used to popularize MHL among university undergraduates and their instructors, interaction through online and face-to-face options with the learners inspired support for mental health. The educators’ attitudes are likely to change during the lecturing process and change the overall mental health stigma (Farrer et al., 2015). This study found a high MHL level among academic advisors who were extremely apt to deal with learners with mental health difficulties. From the researcher’s perspective, this result indicates that most academic staff can handle different mental health issues faced by students due to the individual academic advisor’s specialty in the health field. Most can identify mental health issues and understand the underlying factors of mental illnesses related to their experience in the deterrence and care of mental health complications. The outcome aligns with the conclusions of previous studies implemented by Gulliver et al. (2019), who reported that academic staff had an elevated level of MHL.
Conversely, a study conducted in Pakistan by Khan et al. (2018), which involved a sample of 251 academic staff in a university setting, found that the academic staff had a moderate level of MHL. The researchers found that most laypeople have a poor understanding of medical knowledge. Such people cannot correctly recognize mental illnesses and understand the underlying causal factors of mental illnesses. However, a study conducted by Aluh et al. (2018) in Nigeria among 120 teachers in high schools found that their mental health literacy was low. This finding found that instructors cannot identify learners with mental health problems and refer them to the appropriate mental healthcare professionals.
With regard to the academic advisors’ experience dealing with students’ mental health difficulties, it was revealed that the most commonly mentioned experiences in such instances were “having previously taught a student with a mental health problem”, followed by “feeling sufficiently informed to respond appropriately to a student with a mental health problem”, and “being approached by a student to discuss their mental health” and “initiated a conversation with a student to discuss their mental health”. The least common experience mentioned by academic advisors was “student experiencing suicidal thoughts”. This result may be because of students’ feelings of shame about seeking help if they have suicidal thoughts. These results reflect the academic advisors’ experience of different circumstances when interacting and initiating conversations with learners or when being approached by students for support. This result is in agreement with the results obtained by Hernández-Torrano et al. (2020) found that the mental well-being of university students with mental health problems depends on their interactions with the university staff. Additionally, teaching and receiving mental health information shapes understanding of other predictors of mental health problems, such as substance abuse, mental disorders, stigma, and stress. Academic advisors rely on the knowledge of mental health problems to advise students on how to seek counseling or a mental health consultation outside the college.
Experience and professional roles shape academic advisors' knowledge, recognition, and positive attitudes toward students with mental health problems. These may vary according to gender, years of experience, and teaching roles. This engagement builds confidence and leads to conversations that translate into effective treatment and recovery of the students. The findings are consistent with several findings affirm the high level of MHL and the subsequent effectiveness in handling different mental health problems affecting students. Xu et al. (2018) established that help-seeking by undergraduates was effective in improving knowledge, attitudes, and positive intentions toward their mental health problems. Furthermore, Svensson and Hansson (2016) found that MHL shapes the experiences of the academic staff, who then establish a relationship with family members and students. A high MHL is an effective anti-stigma intervention and tool for reducing social distance between students with depression, psychosis, or stress and their academic advisors.
Implications of the Study
The outcomes of this study have implications for healthcare in general and nursing practice in particular at national and international levels. Nationally, policymakers should develop continuing education programs for healthcare faculty, including nurses, to improve their familiarity with common mental health issues and increase their mental health literacy (MHL). In addition, academic advisors should be trained in mental health first aid to raise awareness on responding to students with mental health issues. Furthermore, policymakers should lobby for additional funds from the national government to undertake campaigns to improve MHL at the community level.
Internationally, health science sectors, including nursing, should develop mechanisms for combating mental health stigma and misconceptions among academic advisors. The process of handling mental health issues among students exposes the advisors to mental health challenges. The initiative at a global level requires multi-stakeholder input to create wellness programs, enhance self-management, and institute counseling training and certification for academic advisors dealing with students with potential mental health issues.
Limitations
This study had some drawbacks. The research adopted a cross-sectional study model, and the data were collected at a particular time. With a dearth of studies assessing the MHL among academic advisors at university levels around the country, no comparative data was available. Moreover, academic advisors were recruited in just the health field campus in one university, limiting the generalizability of the finding. Thus, the results might not represent academic advisors at other universities.
Conclusion
This study set out to assess academic advisors’ MHL and their experiences when dealing with students facing mental health problems. A descriptive cross-sectional approach was adopted for the study. A total of 133 academic advisors participated in this study. This study found a high level of MHL among academic advisors when dealing with undergraduates with mental health complications. The respondents’ age, gender, and years of experience did not significantly affect the levels of MHL in this study. However, a greater level of MHL was linked to higher experience among academic advisors dealing with students' mental health problems.