










Background
In order to monitor and control infections in hospitals, a special nurse called the Infection Prevention and Control Nurse (IPCN) is employed. This nurse is part of the infection control professionals, also known as Infection Preventionists (IP). The IPCN plays a critical role in preventing Healthcare Associated Infections (HAIs), also known as nosocomial infections. These infections occur in patients during treatment in hospitals or other healthcare facilities and are not present during admission or incubation (World Health Organization, 2002). In addition to advocating for and implementing infection control practices (Freeman & Gray, 2013; Kalp et al., 2018; Liu et al., 2014), the IPCN brings a vision of discipline, reinforcement, responsibility, and high dedication. This vision serves as a constant driving force in preventing and controlling hospital infections (Assariparambil et al., 2021; Vassallo & Boston, 2019).
Improving competence in controlling the risk of healthcare-related infections in hospitals has proven to be a challenge for IPCNs. This is due to the complex nature of Infection Prevention and Control (IPC), which involves various factors, such as environment, microbiology, pathology, human error, systems, and organizations (Freeman & Gray, 2013). Furthermore, IPCNs are required to think quickly and critically in response to rapid changes. Therefore, organizations are expected to support and encourage IPCNs to enhance their education, work experience, and performance based on their competencies (Gase et al., 2015).
In an effort to maintain their competence, IPCNs are required to attend continuing education, develop new skills, and stay up-to-date with current infection control practices (World Health Organization, 2018). IPCNs possess expert skills and competencies that can help organizations increase staff engagement, productivity, and satisfaction. IPCNs can motivate staff to work more effectively, improve performance, create networks, and be proactive in improving services, making the staff feel valued (Aziz, 2016). IPCNs carry a heavy workload in implementing infection control programs, which is critical for patient and staff safety and service quality.
During the COVID-19 pandemic, this responsibility is even more challenging as it requires strict infection control measures. IPCNs visit high-risk patients, monitor the implementation of infection control programs and Standard Operating Procedures (SOPs), audit isolation precautions, provide education to patients and staff, and investigate healthcare-associated infections (HAIs), as stated in the Regulation of Ministry of Health number 27 of 2017 (Ministry of Health, 2017). IPCNs functionally report to the Infection Prevention and Control Committee and professionally report to the Nursing Committee at the same level as senior managers.
However, the healthcare industry is continuously changing, with an increase in infection cases leading to stress and potential burnout for IPCNs (Colindres et al., 2018). They face various challenges such as role conflicts, work overload, lack of personnel, institutional pressure, inadequate knowledge about infection control, and lack of support from nursing organizations, all of which increase the risk of turnover (Choi & Kim, 2020; Diño et al., 2022). A psychosocial work environment lacking appreciation and balanced rewards also reduces nurse adherence to preventing and controlling infections (Colindres et al., 2018). Unfortunately, IPCNs in Indonesia may still face these phenomena and issues with leadership support, facilities, infrastructure, and rewards.
Therefore, this study aimed to explore IPCNs’ current experiences in performing their roles and duties in hospitals to recommend measures to improve their performance in preventing and controlling hospital infections.
Methods
Study Design
This qualitative research applied a qualitative descriptive study design. Qualitative descriptive study is typically based on naturalistic inquiry, which involves studying a phenomenon in its natural state to the fullest extent possible within the research context. This means that study variables are not pre-selected, there is no manipulation of variables, and there is no prior commitment to any particular theoretical view of the phenomenon being studied (Lambert & Lambert, 2012). With this method, participants’ opinions or views about their experiences regarding their roles and duties in the hospital, the obstacles faced, organizational support, and IPCN’s expectations of their careers were explored and reported.
Participants
The study participants were all full-time IPCNs who served on the Infection Prevention and Control Committee. Six female participants were selected through purposive sampling, which ensured they had similar characteristics and work experience (aged 41-52 years with 3-12 years of work experience). None of the participants refused to participate or dropped out. The inclusion criteria required that participants work full-time at the hospital’s Infection Prevention and Control Committee, have a minimum of one year of work experience as an IPCN, and have basic/advanced/IPCN training certification.
Data Collection
Data were collected in April 2021 through a 120-minute Focus Group Discussion (FGD) at the Gatot Soebroto Army Central Hospital (RSPAD), Jakarta, Indonesia. FGD was used to explore specific issues to provide valuable information from groups of participants who interact with each other by expressing their thoughts, feelings, and experiences (Holloway & Galvin, 2010). The FGD was held in the Infection Prevention and Control Committee meeting room at the hospital. The data were audio recorded with the participants’ consent. The discussion began with the question, “What are your roles as an IPCN, and how do you perform these roles?” During the FGD, participants were also asked about their opinions regarding constraints, work environment, management support, and career development. The researchers validated all answers, observed non-verbal expressions, and asked probing questions to obtain meaningful words or views.
Data Analysis
The data were analyzed using thematic analysis of the FGD transcript, which looks at qualitative data analysis as a process that requires sequential steps to be followed, from the specific to the general (Creswell & Creswell, 2018). This process consisted of six steps: data preparation for transcription, reading of the entire data, detailed data analysis by coding the data, description of categories, definition of themes and interpretation of data, and preparation of a qualitative report. The transcript of the FGD was read, analyzed, and then described in keywords to be further discussed by the research team simultaneously to determine the categories and themes.
Trustworthiness
The researchers conducted member checking to ensure the validity of the search data. After obtaining the themes of the results of the data analysis, validation was carried out with all participants. All participants confirmed that they experienced the themes found based on the validation results. Next, the researchers carried out thick descriptions by writing down variations in participant characteristics to ensure that the results could be applied to a population with the same background. The researchers also conducted a peer audit with the research team to identify the accuracy of the research result in themes based on interview data. In order to enhance the study rigor, the research team conducted peer reviews at each stage, with all members participating. The team then cross-checked and validated the data to ensure that the findings were accurately allocated and matched to the relevant sub-themes and themes, reaching a consensus.
Ethical Considerations
Prior to participating in this study, all participants received information on the research objectives, procedures, duration of involvement, participant rights, and forms of participation and provided their consent by signing an informed consent form. Furthermore, this study underwent ethical review by the Research Ethics Committee of the University of Indonesia and was approved under number KET 214/UN2.F12.D1.2.1/PPM.00.02/2022.
Results
Characteristics of Participants
The participants in this study were six full-time IPCNs in the IPC Committee, aged 41-52 years and with 3-12 years of work experience. One participant (17%) held a master’s degree in clinical epidemiology, while the other five (83%) had a bachelor’s degree in nursing. Each participant was assigned a code number (P1-P6). Table 1 presents the characteristics of the participants.
| Code | Sex | Age | Education | Length of Service |
|---|---|---|---|---|
| P1 | Female | 43 | Master’s Degree | 12 years |
| P2 | Female | 48 | Bachelor of Nursing | 5 years |
| P3 | Female | 43 | Bachelor of Nursing | 4 years |
| P4 | Female | 41 | Bachelor of Nursing | 4 years |
| P5 | Female | 52 | Bachelor of Nursing | 4 years |
| P6 | Female | 45 | Bachelor of Nursing | 3 years |
Thematic Findings
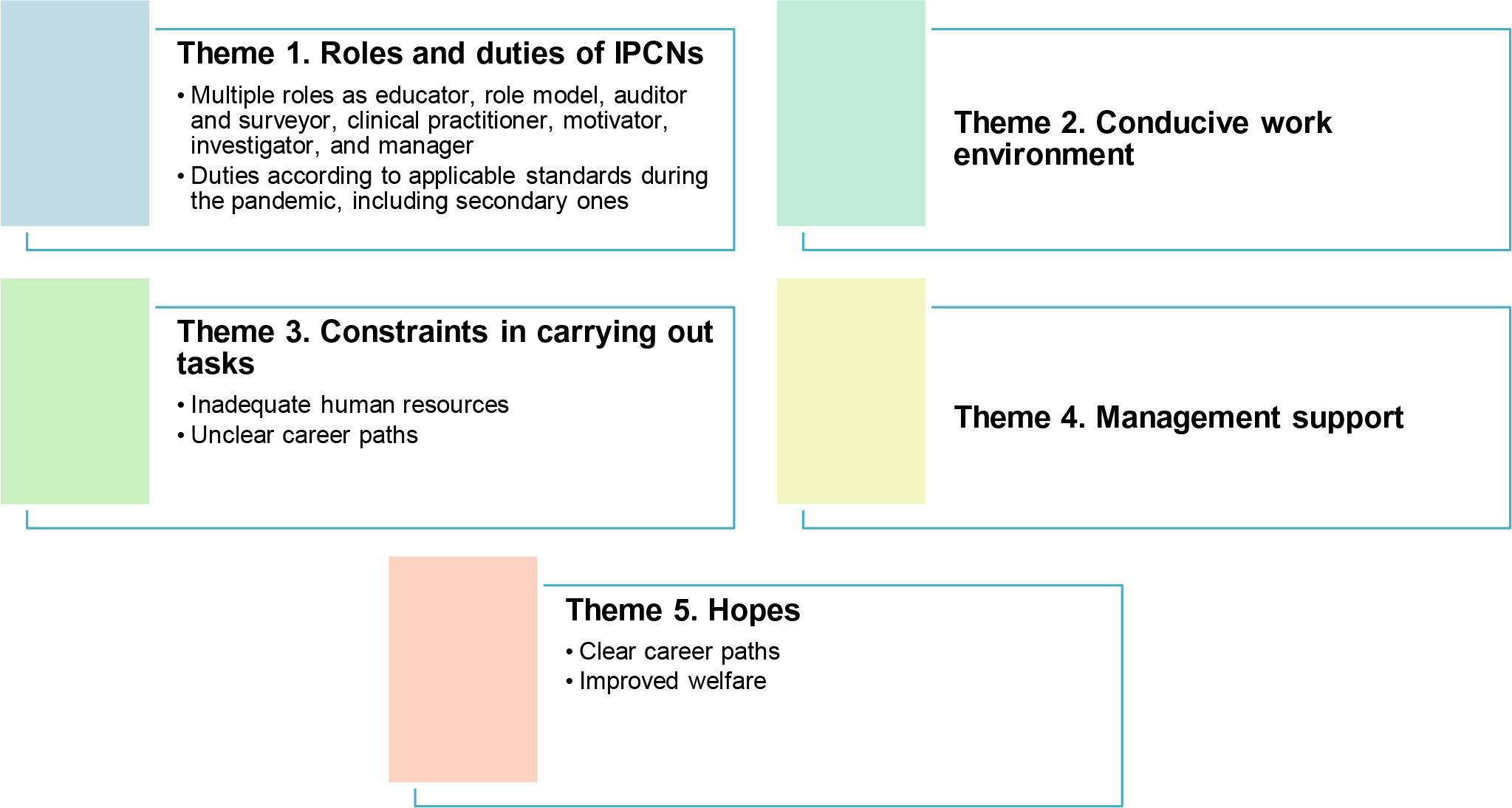
Five themes were identified: 1) primary and secondary roles and duties during the COVID-19 pandemic, 2) conducive work environment, 3) constraints in carrying out tasks, 4) management support, and 5) hopes (Figure 1).
Theme 1: Roles and duties of IPCNs
Subtheme 1.1: Multiple roles as educator, role model, auditor and surveyor, clinical practitioner, motivator, investigator, and manager
Of all participants, four IPCNs answered that they performed their role as educators.
“… so, my role there is as an educator… providing education related to the SOPs.” (P3)
“… disseminate policies and SOPs to the heads of installations, covering inpatient installation and outpatient installation, then to the department.” (P1)
“… our roles as educators …” (P6)
“… yes, for education … how to comply with health protocols …” (P2)
Furthermore, two of the six participants mentioned that they became role models.
“… IPCN as a role model, we continue to evaluate all activities, whether they are in accordance with the SOP or not …” (P1)
“her role as a role model … how to maintain health protocols…” (P4)
Four of the six participants responded that they had the roles of auditors and surveyors.
“Our roles as auditors and surveyors on the wards enable us to detect extraordinary events …” (P1)
“… I monitor … I evaluate how the PPE is used …” (P3)
“… IPCN in this vaccination is monitoring, one of which is monitoring AEFI; this is the role of IPCN in vaccination activities.” (P4)
“Monitoring and evaluation; how nurses adhere to audit bundles” (P6)
In addition, four of the six participants stated they served as clinical practitioners.
“… IPCN as a clinical practitioner … early detection of HAIs … monitoring symptoms, medical records, culture results … mastering diagnoses, signs, and symptoms …” (P1)
“… postoperative patients who underwent surgery, how are the HAI bundles, how are the surgical bundles …, pre-, intra-, and post-surgery …” (P3)
“Detection of ESBL or MRSA culture results …” (P4)
“… patients with ventilator installed, how are their oral hygiene … catheter inserted … whether it is properly placed or not. Not on the floor.” (P5)
Three of the six participants answered that they played a role as motivators.
“… as a motivator to maintain the spirit of implementing health protocols.” (P2)
“… yes, as Infection Control Nurses, our duty is to motivate …” (P3)
“… we as motivators, Ma’am, … when our colleagues are feeling bored, having a meltdown due to exhaustion, the pandemic and isolation are at a high level, that …” (P5).
Three of the six participants also acted as investigators.
“So, the role of IPCN is to detect early outbreaks (extraordinary events) and infectious diseases such as diphtheria …” (P1)
“… role in tracking …when there is a patient who has close contact with the patient.” (P5)
“… As investigators, we also carry out the 3T, namely Tracking, Test, and Treatment, if there is a positive result.” (P6)
Meanwhile, two of the six participants believed they performed the role of managers.
“… as a manager through coordination with superiors …” (P1)
“… as managers, Ma’am… we coordinate with relevant parties at the top levels and parallel levels …” (P2)
Sub-theme 1.2: Duties according to applicable standards during the pandemic, including secondary ones
All participants stated that their duty was to conduct surveys around the treatment wards.
“Field monitoring, … whether … our colleagues comply with IPC [measures and standards] …, conduct initial investigations on HAIs, monitor … the implementation of bundles, …” (P1)
“… around according to their respective areas” (P2)
“We go around the treatment wards to do surveys, …” (P3)
“We monitor … ward temperature and humidity.” (P4)
“We do 5R supervision … related to HAIs.” (P5)
“Ward infection control … audit bundles, … monitor ward cleanliness” (P6)
Three of the six participants had a duty to establish policies and IPC SOPs.
“We have to establish policies and SOPs so that our colleagues in this field do not follow all procedures in the hospital …” (P1)
“… doing what is called additional job, that is SOP-making.” (P2)
“… coordinating inpatient ward management policies with the heads of affairs, sub-divisions, or installations…” (P3)
Two of the six participants carried out their duties in providing education.
“… to educate patients in polyclinics about how they can prevent …, comply with health protocols” (P2)
“… IPCN gives education to both patients and visitors or even internally to our colleagues …” (P4)
Additionally, two of the six participants informed their duty of monitoring the Infection Control Risk Assessment (ICRA).
“Monitoring ICRA … to develop work programs and … to assess the risk of infection” (P1)
“… monitor ICRA …” (P6)
Three of the six participants revealed the duties of making HAIs reports and recommendations.
“Making HAIs reports, audits … and recommendations” (P1)
“… Make a HAIs report, hand hygiene report, PPE, HD …” (P2)
“We made a report of the officer’s needle piercing…” (P5)
Furthermore, four participants stated they had additional duties to give vaccines and prepare COVID-19 reports.
“… due to the pandemic, there is a special report on COVID-19” (P1)
“… extra assignments, additional duties, vaccinations, and COVID-19 reports” (P2)
“… reports on our employees infected with COVID-19 …” (P3)
“… there is an additional duty as a vaccinator … as a PIC, report to the superiors” (P6)
Theme 2: Conducive work environment
Five participants reported a supportive work environment.
“… our environment in this IPC Committee is warm and not problematic …” (P1)
“As for the environment …. we are all fast respond” (P2)
“… thank God … all of our colleagues here are loyal, Ma’am… willing to take the time, prove our outputs to everyone.” (P3)
“… we do a lot for the good of everyone. That’s the principle, … so… pretty calm” (P4)
“… enjoying the work … loving our work” (P6)
Four of the six participants stated they were accepted and recognized in their work environment.
“… we have involved the SOP, flow, zones, and PPE in the treatment ward” (P3)
“… in the ward, has been a little accepting, and we’re involved” (P4)
“We record the output data … we develop a policy … we can solve … a problem … that’s motivational” (P1)
“We are selected people who have different knowledge … from our colleagues” (P6)
Three participants believed that they worked in a challenging environment.
“The environment is very dynamic …” (P5)
“The demands are high from the superiors … the authority is high, and then … our colleagues … also never give up” (P1)
“In the field of supervision, it is full of challenges. Because we are facing a lot of colleagues and characters … in the ward” (P6)
Theme 3: Constraints in carrying out tasks
Subtheme 3.1: Inadequate human resources
Five of the six IPCNs revealed the constraints of inadequate IPCNs, overtime, and workload.
“… lacking IPCNs, Ma’am.” (P3)
“… sometimes we work overtime … on the other hand, sometimes those who are in the ward … think that we’re only taking data … and chatting” (P2)
“Control Team … the pandemic … being a call-center staff for COVID-19 as well … taking care of the coordinator … taking care of the unit … (extra job)” (P1)
“… during the pandemic, we also conduct tracking … becoming vaccine coordinator” (P4)
“We have already been in the field too, writing … means of reporting that processes the data, we did that too.” (P6)
Subtheme 3.2: Unclear career paths
One participant revealed that the career path and competency test for IPCNs were equal to those of clinical nurses in the ward.
“We are … still … adjusting … the level increase … and our careers are like nurses in the ward … Yes … our competency test … is still … the same as nurses in the ward” (P5)
Theme 4: Management support
Three of the six participants stated they received support in facilities and infrastructure.
“For us personally during this pandemic, leaders also play a very important role in giving vitamins” (P4)
“The leaders play a very important role in the administration of vitamins … snacks …” (P5)
“… for the facility in the form of PPE and office stationery … equipped with Wi-Fi.” (P6)
Three of the six participants also gained recognition and authority of work.
“… give authority … support us from behind by providing backups” (P1)
“… we started to feel that we are recognized as IPCN” (P2)
“… equal welfare with the head of the ward …” (P3)
Theme 5: Hopes
Subtheme 5.1: Clear career paths
Two of the six IPCNs expressed their hopes for the competency test for IPCNs.
“… our career path is not the same as that of nurses in the ward … functionally, IPCNs’ duties and responsibilities still follow the clinical nurses.” (P1)
“… yes, maybe in the future our career path is not the same as that of ward nurses … specifically for IPCNs themselves … What is their career path? … that is … our hopes are like that …” (P2)
Meanwhile, four participants hoped for a career path based on competency improvement.
“…our hope is that in the future our careers can develop, taken into account because of our leading role” (P3)
“… able to develop … promotion … for example, we are IPCN … yes, but not only that. IPCNs have knowledge … our knowledge has levels” (P4)
“… initial recruitment … what kind of increase … it can also be of the level … can also be with other awards … which already … over 10 years … how … those are what we hope for.” (P5)
“Competency test according to management … we are independent as IPCN … that’s the point … specific according to IPCN hopes” (P6)
Sub-theme 5.2: Improved welfare
Two of the six participants expressed their hopes for an increase in IPCN remuneration.
“… our hope … for welfare beyond the Head of the Ward …” (P3)
“… and the benefits also increase … according to their role and duties” (P5)
Furthermore, two of the six participants hoped for more IPCNs based on workload analysis.
“… hope to increase the number of IPCNs per accreditation regulations, and nationally, 100 beds need one IPCN, whereas we have almost 800 bed or more … need two more IPCNs” (P1)
“Actually, the crucial thing is the support of colleagues.” (P3)
Discussion
All participants in this study reported on the roles of IPCNs in the IPC Committee, which are performed and adopted as guidelines in their daily work. The most prominent roles are as educators, auditors, surveyors, and clinical practitioners. Every day, IPCNs facilitate health workers to socialize policies and SOPs, regularly conduct round-the-clock monitoring of treatment wards, and supervise IPCLNs to monitor clinical practices in implementing HAIs bundles. This is followed by their roles as investigators in detecting extraordinary events or tracking cases and motivators in implementing health protocols and encouraging health workers to comply with IPC standards and measures.
In addition to these roles, some participants stated that they also serve as role models and managers. This is in line with a statement of Aziz (2016) that IPCNs have negotiation skills and abilities to provide education, become role models, carry out complex decision-making, and have leadership and management skills to motivate staff to improve performance, expand networks, and be proactive in improving services.
In addition to their roles, all participants revealed their daily duties, the most notable of which was conducting surveys in treatment wards. Other duties widely carried out by IPCNs include establishing policies and SOPs, preparing HAIs reports, and making recommendations. Several participants also had a responsibility to monitor ICRA. During the pandemic, IPCNs have additional duties of providing vaccines and reporting on patients with COVID-19. This is in accordance with the results of a prior study by Popescu (2019), which stated that IPCN’s duties and responsibilities include supervision, investigation of infection-related cases, staff education and research, policy review, infection risk assessment, emergency preparedness, hospital infection reporting, and recommendation making. In addition, IPCNs have a vital role in communication, especially in high stress and anxiety about the COVID-19 pandemic, which increases the risk of transmission for nurses (West, 2021).
Most of the participants expressed that there was leadership support for implementing their daily work. This is supported by the acceptance from the ward, as well as the openness and involvement of IPCNs in managing infection services in treatment wards, which can encourage confidence in performing their roles. This is consistent with a previous study by Reisinger et al. (2017), which found that competencies strengthened by environmental support will increase self-confidence and commitment to implement these competencies in standards of practice.
All participants felt motivated after being given authority and the ability to solve problems and prove that their work benefited many people. In addition, they felt special with their distinct knowledge, which made them do good work and enjoy and love their work. Such support lifted their spirits, increasing their dedication and professional performance to improve service quality and job satisfaction. This is in line with Bernard et al. (2018), who proved that IPCN’s work motivation would increase the satisfaction of continuous innovation that encourages the improvement of organizational performance and goals. Well-maintained motivation would provide satisfaction for their achievements. Meanwhile, research conducted by Platace et al. (2020) identified that non-material factors have a greater influence on IPCN work motivation, such as a high sense of responsibility and concern for patients, colleagues, and their safety.
Furthermore, the participants highlighted the constraints related to the lack of IPCN, the advancement of IPCN career paths, and the IPCN competency test, equated with that of nurses in the ward. As mentioned above, IPCN has different duties and responsibilities, as well as a broader scope of area and level of problems encountered. Therefore, insufficient IPCNs affect unbalanced, extra, or redundant work performance. This is in accordance with a prior study by Mugomeri (2018), which stated that human resource support greatly affects the effectiveness of IPCN performance, reducing unclear competencies and roles. This is also emphasized in the Regulation of the Minister of Health Number 27 of 2017 (Ministry of Health, 2017) on IPCN personnel standards, where one IPCN is in charge of 100 beds according to the level of needs and the risk of infection in the hospital.
Regarding IPCN career paths, competency-based career development can be encouraged through a specific competency test done periodically to increase levels based on the competency domains specially formulated for IPCNs who work full-time (Billings et al., 2019).
All participants stated that they received support from their superiors in carrying out their duties as IPCNs. Their superiors gave authority, support, backups, recognition, and welfare, as well as equip them with adequate facilities and infrastructure. This will provide IPCNs with comfort, eventually leading to job satisfaction and self-confidence. According to Yoon et al. (2016), human resources who play a role in the effective implementation of IPC programs need management support. Likewise, Mugomeri (2018) argued that the ineffectiveness of IPC organizations in controlling infections is influenced by ineffective organizational support.
Concerning the IPCN’s hopes, all participants hope to advance the IPCN career path according to their roles and responsibilities, which can be developed by taking into account their prominent roles in preventing and controlling infections. They also expressed their hopes for recognition and appreciation that correspond to their work, length of service, and level, followed by increased IPCN welfare. This is aligned with a study by Knighton (2020), which argued that analyzing the incentive programs received along with the performance improvements described in career development in the form of financial support is necessary. Therefore, the criteria for awarding compensation are related to experience, education level, certification, and performance improvement according to their career path.
In addition to financial support, competitive salary spurs career development and certification, lowering turnover rates. Likewise, Billings et al. (2019) clarify the roles and responsibilities of IPCNs and guide their career development, identify and design their career paths, and accurately reflect their roles and responsibilities in collaborating, communicating, and consulting with other parties in efforts to develop their competencies.
Conclusion
This study provides current insights into IPCN’s roles and duties that require collaboration and coordination with multi-professions, as well as management support to overcome barriers and challenges that hinder the fulfillment of responsibilities and hopes of improving IPCN performance following competency-based career paths to achieve patient safety, service quality, and job satisfaction. In addition, the findings may be served as basic information for future studies to measure IPCN roles and responsibilities and develop interventions to improve their skills and performances.