










Background
Advancing public hospitals to provide current services to the public necessitates the full participation of nurses from all departments. The involvement of nurses can be manifold, but the most vital and pressing issue is acknowledging nurses’ experiences which later formed into meaningful ideas for publicly funded hospital progress without compromising the standard feasible hospital daily operations. Public speakers, thinkers, scholars, and business leaders speak loud about present living environments, which are highly unpredictable, inexact, and multifaceted. Thus, the power of expression directed to general and specific misalignment of hospital-related innovation should be inevitably in practice. It is likely essential for nurses to remain focused while handling health care and management demands, similar to the reasoning in business organizations (Mowbray et al., 2021; Su et al., 2017). We have realized that the nurses act as the foreheads that induce directions for the hospitals thru knowledge sharing gathered from the stakeholders, particularly patients. If nurses decide not to or withdraw from expressing their concerns about innovative hospital practices and other organizational behavior glitches will marginalize opportunities for error detection, provision of solutions, and strategic implementations to avoid silent workplace unproductiveness and performance to the highest expectations (Kim & Ishikawa, 2021). Besides, the hospital management probably delays making vibrant decisions, improving department functioning, and sustaining hospital organizational efficiency (Hussain et al., 2019). Perhaps these will knock down their reporting to the public on managing entities with public funds. Thus, hospital management needs to place measures to nurture nurses’ continuous support in voicing their experiences and thoughts while performing their daily routines, fulfilling stakeholders’ interests, and attaining the hospital and national healthcare services missions.
The study on voice behaviors is gaining continuous support across the research disciplines. Despite numerous perspectives, characteristics, and definitions available, for easy understanding, voice behavior is voicing concerns and thoughts for improving a situation (Morrison, 2014) or improving the service management system with required innovation from the hospital context. According to Dyne et al. (2003), speech is a tool for change-oriented communication and can improve otherwise dismal conditions. Van Dyne and LePine (1998) categorized vocal behavior as promoting or inhibiting. Voice behavior supporting employee suggestions for strengthening organizational work processes is promotive and must be continuously encouraged at all levels (Kakkar et al., 2016) and occasionally mistaken that promotive voice as a challenge to the authority of the organization’s management since it provides possibilities to alter the status quo of the personnel (Chen et al., 2018; Engemann & Scott, 2020).
When nurses use prohibitive voice behavior, they are concerned about the workplace and have a chance to explain the potential hazards. Prohibitive voice behavior seen as favorable is proactive and focused on the future. Unacceptable speech patterns glance ahead or back. Voice-related actions go above and above to improve creativity and productivity and reduce errors at work (Morrison, 2014; Van Dyne & LePine, 1998). Inconsistent in-role behavior or disdain for one’s duties in one’s allotted position will result in unfavorable monetary sanctions and lost possibilities for promotion (Van Dyne & LePine, 1998). Consequently, many nurses facing difficult situations might choose to be silent. This condition needs to be continuously studied, and best practices learned and implemented in hospitals that are serious in curbing malpractices while advancing healthcare provisions for the betterment of humankind.
Leadership is crucial in allowing nurses to constructively express their thoughts, agreeing with earlier pragmatic studies (Hsiung, 2012; Jada & Mukhopadhyay, 2019; Yan, 2018). However, despite these advancements in voice research, further investigation is essential to determine the underlying psychological mechanisms in leadership that influence nurses’ or other employees’ voice behavior (Engemann & Scott, 2020; Lam et al., 2018; Morrison, 2014).
One of this paper’s intended outcomes is to suggest the significance of psychological security and underlying motivation drive in foreseeing nurses’ voice behavior. The foundation of the social exchange theorem propagated by Blau (1964) entails believing that leader and member reciprocity will yield healthy behaviors in the workplace. Corresponding to this theory, employees’ positive impressions of the organization’s treatment of them led them to express concern for the best practices that benefit all. Nurses are much more apt to speak their minds in conditions where they know they are protected and can trust the safety of those around them. So, it is the responsibility of hospitals to shield their nurses’ hearts and minds. Psychological safety means the employees do not worry about how others may see them professionally or personally (Kahn, 1990).
There is a strong desire for empirical evidence supporting the connection between leadership and voice behavior. Vocal behavior is recognized widely as a crucial facet of employees’ citizenship behavior that complements multifaceted performance and hospital organizational development. Management is often put in danger by unresolved problems at the workplace. Intrinsically motivated nurses do what they do because they enjoy it, not because they hope for some external rewards (Deci & Ryan, 1985). Scholars have researched and reported a positive connection between an intrinsic member of staff motivation and performance in several contexts. Therefore, it is crucial to determine if empowered leadership can affect employee voice behavior by boosting innate motivation drive.
Indirect Effects of Psychological Safety
Clark (2020) defines the concept of psychological safety as the absence of worry about being ridiculed, excluded, or reprimanded because of one’s opinions or actions. A greater sense of comfort and lack of perceived risk, Kahn (1990) posited to increase employee responsibility. Searching the history, we note that Schein and Bennis (1965)’s research on organizational change explains that psychological safety increases chances for employees to take risks since they feel safe and capable of handling the consequences. Psychological safety is essential in simplifying thoughts and behaviors in any organization, particularly in group concentration phenomena (Edmondson & Lei, 2014). Therefore, it is critically important in managing the public hospital. Psychological safety in healthcare settings improves patient outcomes by encouraging nurses to report errors and participate in quality improvement initiatives (O'Donovan et al., 2021). Team members who offer constructive criticism of the hospital’s performances think through the repercussions of their actions before voicing them. They worried that others would misunderstand or reject their offer. These are common in organizations that do not encourage open dialogue and inquiry. However, Dutton et al. (1997) note that employees sometimes incorrectly judge whether it is safe to speak up. In this situation, confused nurses probably remain silent instead of actively engaging in voice behavior, knowing at the same time they are protected in the event of speaking up their minds (Detert & Edmondson, 2011). It is popular in the social science studies repeating Morrison (2014), who asserts that the opinions and actions of managers (in the context of a hospital, head nurse) significantly impact whether or not workers participate enthusiastically in voice behavior and make it part of the hospital culture.
Nurses are more likely to use their voices in a positive work environment. The hospital culture also plays a significant role in encouraging nurses to raise concerns about their work. One way to build hospital employees’ psychological security is to have an approachable and open leader (Edmondson & Lei, 2014). The hospital department leaders can learn what nurses and other employees think and feel about workplace practices and encourage them to voice their opinions without any restrictions. Whistleblowing can happen positively within the hospital for progressive improvement, and most importantly, stakeholders’ interests are well taken care of.
Nurses must also be confident that voicing their opinions will have no negative consequences. Rules, regulations, and procedures should be in place for all nurses to be comfortable, making voice behavior a standard norm in the hospital. When strong leadership exists, it fosters effective cultural practices within an organization (Schein & Bennis, 1965). Earlier research (Liu et al., 2021; Liu et al., 2017; Lu & Lu, 2020) indicated a significant leader-voice relationship mediated by psychological safety. Indeed, Leader-Member Exchange (LMX) philosophy (Graen & Uhl-Bien, 1995) alleges that superiors and direct reports have strong ties.
Hence, the first research hypothesis for the study is H1: psychological safety significantly mediates the link between empowering leadership style and the voice behavior of nurses.
Interestingly, long ago and significant to note that Katz and Kahn (1978) argue that organizations cannot succeed in their missions, produce quality work, or cooperate effectively unless there is a strong network of interpersonal relationships within the organization thriving for excellence (Carnevale et al., 2017). Nurses who form closer relationships with their superiors (substantial LMX relationships) are more open to contributing opinions and putting in the time and effort required to address workplace challenges because they are assured more trust and freedom. The leader is responsible for making the workplace safe for nurses to open up about their emotional well-being in two-person teams. Psychological safety with dynamic team relationships entails more awesome voice behavior and breaks the unhealthy silence among employees who prefer energetic, supportive, and productive work settings and organization growth strategies (Bienefeld & Grote, 2014; Brinsfield, 2013; Xue et al., 2020). Nurses with high psychological safety were presumed to express disagreement wisely, be brave in engaging with open criticism, and be bold in meeting and voicing out their immediate superior or the higher authorities if the lower management remains neutral. Consequently, the following hypothesis formed, H2: psychological safety significantly mediates the link between LMX and the voice behavior of nurses.
Indirect Effects of Intrinsic Motivation
People are intrinsically motivated because they value engaging in novel and challenging activities (Ryan & Deci, 2000). A person who is intrinsically motivated does what they do because they enjoy doing it and are interested in the task at hand (Conchie, 2013; Ryan & Deci, 2000). Employees’ favorable sentiments and overall sense of comfort might be a starting point for self-determination theory, which contends that sovereignty, capability, and affinity increase intrinsic motivation (Deci & Ryan, 2010). As a theory of motivation, intrinsic motivation has recently emerged as a critical factor in employees’ propensity to engage in creative problem-solving on the job. Leaders who excel at empowering their teams do so by delegating responsibility, giving employees a voice in critical decisions, and showing faith in their ability to tackle complex projects (Ahearne et al., 2005). It follows that leaders who insist on equitable distribution of authority can inspire employees to tap into their reserves of intrinsic motivation. Leaders who empower their followers do so by giving them more responsibility for making decisions, disclosing relevant information, praising the initiative, highlighting the importance of setting personal goals and providing a process that inspires them. Besides includes everyone in the group while supporting their right to make decisions. In the hospital context, nurses are prone to care for intrinsic motivation and positive organizational citizenship behavior when urged to manage responsibilities independently and decently and be duly liable for related consequences in the cause of performing their tasks within their workstations. Voice behavior is proactive and challenging, and hospitals that value it are more likely to provide their nurses with outlets to showcase their skills and ideas. The intrinsic motivation also includes voice behavior and other forms of positive deviation (Vadera et al., 2013). Furthermore, empirical studies (Conchie, 2013; Wu et al., 2019) have found direct and indirect links between intrinsically motivated individuals and the execution of voice behavior. Therefore, it hypothesized that H3: Intrinsic motivation significantly mediates the association between empowering leadership style and voice behavior of nurses.
Previous research shows several outcomes significantly influenced by LMX (Erdogan & Liden, 2002; Ilies et al., 2007). However, few studies have examined the mechanism that links LMX and employee feedback (Wang et al., 2016). Firmly attached employees are motivated to do an excellent job because they feel they owe the organization for the good treatment they have received. Since voice behavior is a non-standard role, LMX’s high quality makes it simpler to actualize (Song et al., 2017). Strong LMX relationships spur more significant access to information, and the support of leaders toward the employees encourages them to speak up. Thus, the following hypothesis is relevant to test H4: Intrinsic motivation significantly mediates the association between LMX and the voice behavior of nurses.
Hypothetical Groundings
Many empirical and conceptual reports regarding voice behavior are within the theory of social exchange (SET), which is significant. Blau (1964) proposed a simple definition of social exchange in which individuals voluntarily engage in activities motivated by the expectation of receiving benefits from others. This definition describes the interaction between humans and the world around them. According to Scott et al. (2013), social exchange theory explains people’s feelings of inclusion or exclusion significantly shape their perspectives and actions. Data shows that interpersonal contact promotes knowledge sharing. Based on the premise that individuals have an innate need to communicate with and trade with others, social cohesion is crucial to a balanced and harmonious workplace. The research outcomes presented in this paper are grounded in the SET and LMX theories. Scholars such as Cropanzano et al. (2017) posit that SET is among the highly popularly used theory in research frameworks within managerial sciences and other disciplines such as sociology and social psychology.
Key employees of an organization are considered living symbols of the whole because of the strong bonds employees have with the organization. Employees’ attitudes about the organization’s goals toward these individuals reflect how they treat them, so their treatment indicates their attitudes. Another factor to consider is ensuring organizational members feel valued. Consequently, they are more likely to participate in organization-related events that benefit each person (Ilyas et al., 2021; Jada & Mukhopadhyay, 2019; Jung et al., 2020).
Notably, members who had a good experience, which means they will have robust and valuable interconnections forever with the work units reaching holistically to the organization. When people put in the effort to build meaningful relationships with one another, they reap emotional and behavioral benefits, as was found in a previous study (Cropanzano et al., 2003). Some scholars hold that SET harms processes of negative reciprocity, while others argue that it has an impartial or encouraging impact (Cropanzano et al., 2017; Cropanzano et al., 2003). Nurses not feeling pleased in the organization may be less likely to volunteer their time or ideas. Corresponding to the LMX model, influential leaders cultivate various connections with their subordinates. A leader’s actions are individually weighed (Graen & Uhl-Bien, 1995). Managers and employees alike, LMX theory posits, have multiple personas. Extraordinary LMX connections require positive belief, human acknowledgment, mutual authority, faithfulness, similarity, and undertakings of responsibilities and accountabilities (Graen & Uhl-Bien, 1995). Many have acclaimed the vitality of using balanced to superior LMX in improving assertiveness and encouraging employees to use their voices at the workplace (Botero & Van Dyne, 2009). These claims apply to organizations across the industry, including public hospitals. Ponder also that trust between subordinates and superiors is integral to healthy LMX relationships. The associates will likely take notice of their manager if they know that speaking up means losing personal capital or putting themselves in danger (Botero & Van Dyne, 2009).
Employees who feel equality and fair treatment will positively impact the organization by being responsible individuals and standing for the organization’s success (Gigol, 2020). Employee-leaders-organization relationship is utterly related to feeling empowered, accepting responsibilities, dedication, and increased internal enthusiasm to progress in any circumstances on the job and organizational system (Chen et al., 2018; Duan et al., 2017; Lee et al., 2021). The unique individual, a work-related and mutually beneficial effort of establishing partnerships between employees and employers, is part of LMX’s philosophy (Carnevale et al., 2017). The same view is in the opinion of Graen and Uhl-Bien (1995) and also contended long ago by Van Dyne et al. (2008). Employees better understand their leaders’ perspectives and arguments in well-developed LMX interactions. These people are strongly presumed to contribute fresh forward-thinking to uplift organizational performances strategically. Further, members strive to benefit direct superiors and other coworkers. Moreover, studies (Botero & Van Dyne, 2009; Carnevale et al., 2017) have shown that LMX accurately predicts job performance outcomes.
Methods
Study Design
This cross-sectional study seeks to gather data from nurses working in Malaysian public hospitals. With the data set, establishing a model of the interconnectivity of measurable antecedents (empowered leadership style and LMX), significant mediators (psychological safety and intrinsic motivation), and the voice behavior of nurses are the ultimate aims.
Samples/Participants
Staff nurses were selected randomly from the general medical, general surgical, obstetrics and gynecology, pediatrics, and orthopedic wards from seven large government hospitals in the Klang Valley of Malaysia. All the selected hospitals receive government funding and serve the public’s healthcare needs with little or no charges. Besides, the hospitals are large, able to help a higher-density population in the Klang Valley, and, most importantly, sufficiently equipped with modern technologies and healthcare practitioners. This study used Krejcie and Morgan (1970)’s table to determine the appropriate sample. This study’s population comprises 7446 registered staff nurses. Thus, the sample size needed is at least 367 nurses. The researchers inflated the sample size by 10%, resulting in 408 samples. The head nurses of the respective hospitals help deliver the self-administrative questionnaires to the selected nurses who have completed a minimum of a 2-3-year diploma and hold a bona fide license issued by the Malaysian Nursing Board. The final usable and valid survey responses for inclusion in the model and hypotheses testing totaled 366 data.
Instruments
This study used adapted constructs from established survey questionnaires that have multiple items. Thus no single-item measures in the survey instrument. Ahearne et al. (2005) designed a full 12-item scale that facilitated this study to measure empowering leadership style. Based on subordinate views, Liden and Maslyn (1998) initiated a multidimensional LMX construct consisting of 12 related items measuring four independent dimensions: 1. affect, 2. loyalty, 3. contribution, and 4. professional respect, which aid in gathering nurse respondents’ replies on LMX. Edmondson (1999) logically composed a 7-item scale that was appropriate, widely used, and strongly recommended for assessing psychological safety.
The researchers found three items scale significant to assess intrinsic motivation adapted from the works of Amabile (1985) and Tierney et al. (1999). Finally, Van Dyne and LePine (1998) popularized a six-item measurement scale employed in this study to measure the dependent variable, voice behavior. The completed questionnaire included a commonly used five-point Likert scoring scale, with the lowest (1) indicating ‘strongly disagree’ and the highest (5) representing ‘strongly agree’.
As part of the research ethics, researchers communicated and were granted permission by the instrument owners before adapting the items in the present questionnaire. The original measurement items were observed and showed that the reliability coefficients (Cronbach Alpha) exceeded the acceptable standard value of 0.7. The last section of the questionnaire requested the nurse demographic data of age, gender, ethnicity, marital, nursing experiences, and department. Indeed, the final survey questionnaire was examined by three experts for content validity for use in the local context. The researchers did not attempt to translate this study’s survey instrument into other languages. The standard English language used in the original measures is maintained since it is straightforward, easy to understand, and has no issue for the nurses to respond. Hence, the instrument is valid and reliable, considered excellent, and ready for the actual study.
Data Collection
This empirical study uses a cross-sectional survey, and required responses are collected using a structured questionnaire and self-administered. The researchers personally sent the questionnaires to the selected public hospitals. The head nurses were the contact point to help distribute and collect the completed questionnaires from the respondents-nurses in the selected hospital wards. It was the only feasible way to collect data from Malaysian public hospitals. Continuous follow-up with the head nurses finally yielded completed and valid 366 responses, accounting for an 89.71% effective response rate. The data collection process occurred for three weeks in February 2020. It was successfully ended right before the Malaysian government movement control order beginning the second week of March 2020 in response to the COVID-19 pandemic.
Data Analysis
Before data analysis, researchers ensured that the data was reasonably ready for investigation, which involved handling blank responses, coding, and categorizing the data. The preliminary data analysis and descriptive statistics were performed and generated with IBM SPSS Statistics version 26 software for windows. The interrelationships between the study variables weighed with the latest and famous software, SmartPLS 4, for Microsoft Windows. The multi-item measurements suit the reflective measurement model in which the inherent research constructs run the indicators with encouraging high-level intercorrelations. The chosen measures enable a unidimensional structure and robust internal consistency.
The selected software employs a two-stage procedure: i) assessment of the reflective measurement model, which tests the validity and reliability of the measures, and ii) estimation of the structural model, which helps in forming the final model and to examine the research hypotheses. Hair Jr et al. (2021) and many other scholars (Ramayah et al., 2018; Sarstedt et al., 2020) contended that estimating path models using latent variables and their interactions has propelled the popularity of partial least squares structural equation modeling (PLS-SEM) technique, used across the disciplines.
Ethical Considerations
Medical Research Ethics Committee Malaysia approved this study (Approval reference: NMRR-15-129-25990). in seven selected hospitals within Klang Valley, Malaysia. The participants signed the informed consent before responding to the survey. The research objectives and other relevant instructions were briefed and stated in the questionnaire, and the participants received assurance of the confidentiality of the information collected. Furthermore, we ensured no direct interference during working hours; the contact person was the head nurses of the respective hospitals.
Results
Characteristics of the Participants
The survey respondents included 8 (2.2%) males and 358 (97.8%) females. Females consistently dominate nursing, even though it is a norm in recent years for males to pursue nursing. One hundred seventy-one respondents were within the age range of 20-29 years. They accounted for the majority (46.7%) of the sampled responses. The subsequent largest was nurse respondents aged 30-39, with 105 (28.7%) respondents. In the 40-49 age group, 42 (11.5%) respondents, and 50-59 years comprised 48(13.1%) nurse respondents. Most respondents were Malays, with 331 respondents accounting for 90.4% of the sample. 266 (72.7%) respondents were married, followed by the single group, with 99 (27%) respondents. Only a minority declared themselves as widowed (0.3%). Looking at the responses for work experiences, 98 (26.8%) nurses had between 2-5 years of professional work experience, 72 (19.7%) with between 6-10 years, and 64 (17.7%) responded to accumulate more than 21 years and above work experience.
Additionally, 57 respondents (15.6%) had a range of nursing experiences between 11-15 years. Fifty-five nurses, accounting for 15%, had a year or less of work experience. The smallest group was the 20 (5.5%) nurses with solid nursing experiences totaling 16-20 years. These findings showed that most public hospital nurses have extensive work experience. The respondents were from the general medical and general surgical departments, with 100 respondents (27.3%) and 98 respondents (26.8%). Sixty-eight respondents (18.6%) were from the pediatrics and 56 (15.3%) were from the orthopedic department. The least number of respondents were from the obstetrics and gynecology (O & G) department, accounting for 12% or 44 respondents of the samples.
CMB - Common Method Bias
Observing the VIF- variance inflation factor values generated by performing the complete collinearity data diagnostics for scanning issues of CMB is essential. The VIF values ranged from the lowest, 1.139, to the highest, 2.921, which promised that the model of this study was free of CMB. Kock (2017) recommended observing a threshold value of less than or equal to 3.3 to qualify for the claim for free of CMB in empirical research. The complete VIF values for the constructs empowering leadership (EL), leader-member exchange (LMX), psychology safety (PS), and voice behavior (VB) are in Table 1. One of the requirements to test the structural model after fulfilling the conditions for the measurement model is ensuring that the VIF indicators are within the acceptable threshold, which is less than 5.0 (Hair Jr et al., 2017; Ramayah et al., 2018). At this point, VIF values were within the approved range, and no multicollinearity that could jeopardize the assessment of the structural model discussed in the later part of this paper.
| Construct | PS | IM | VB |
|---|---|---|---|
| EL | 1.139 | 1.139 | 2.921 |
| LMX | 1.139 | 1.139 | 1.262 |
| PS | 2.555 | ||
| IM | 1.985 |
Analyzing the Reflective Measurement Model
The measurement model is the first to establish after the testing of the reliability and validity of the latent variables framed for a specific study. Once the measurement model fits the requirements, it enables the functions of the structural model in which the possible associations between the study constructs are analyzed and exposed with statistical facts—decisions on the proposed hypotheses and conclusions made at this stage.
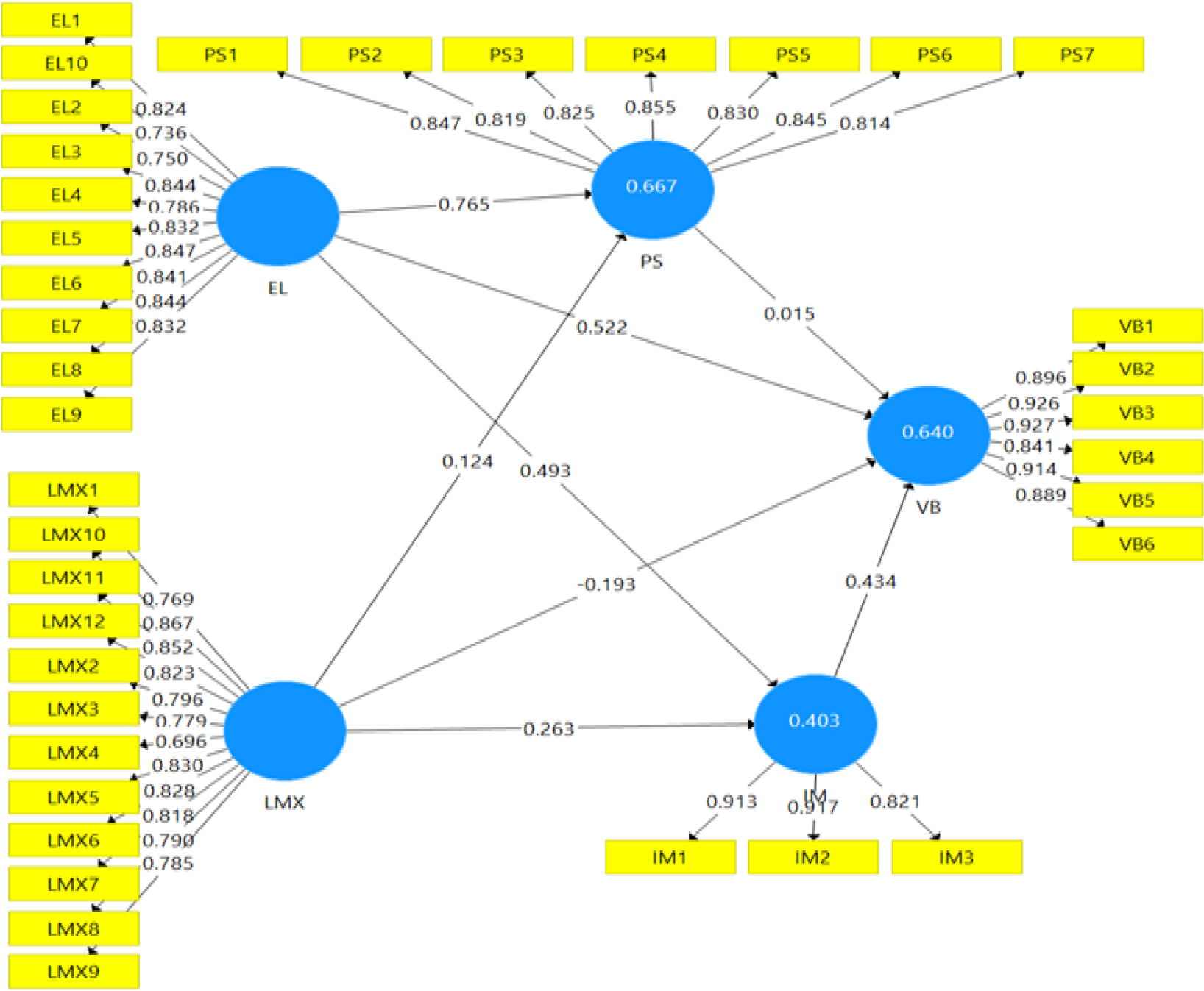
Hair et al. (2019); Hair Jr et al. (2021) provided a comprehensive guide to assess the reflective measurement model and the structural model estimation. The guidelines and suggestions helped make wise statistical decisions for this study. The construct measures reliability was assured by looking at Cronbach alpha (CA) and composite reliability (CR) scores. The statistical indicators obtained from the SmartPLS 4 software showed that the observable values of CA and CR passed the threshold value of 0.7. The convergent validity was assured by observing the importance of the outer loadings and the average variance extracted (AVE). The loadings (see Figure 1) surpassed the recommended threshold of 0.708. And the values of the AVE testing for the convergent validity were more outstanding than the recommended threshold value of 0.50 (see Table 2). In establishing the discriminant validity, assessing values of the Fornell-Larcker criterion, cross-loadings, and Heterotrait–Monotrait Ratio correlations (HTMT) are essential. These three approaches warrant the discriminant validity of the proposed research model. For simplification purposes, in this paper, the HTMT results are reported (see Table 2). All the HTMT correlation values were lower than 0.90, thus passing the standard cut-off point (Hair Jr et al., 2017; Ramayah et al., 2018). The reflective measuring model satisfies all of the requirements for a good fit and therefore enables the assessment of the structural model and testing of the four research hypotheses with PS and IM as the mediators on the test of relationships among EL, LMX, and VB.
| Constructs | Reliability (CA & CR) Convergent Validity (AVE) | Discriminant Validity: Heterotrait-Monotrait Ratio (HTMT) | |||||
|---|---|---|---|---|---|---|---|
| CA | CR | AVE | EL | LMX | PS | IM | |
| EL | 0.943 | 0.952 | 0.663 | ||||
| LMX | 0.860 | 0.915 | 0.783 | 0.363 | |||
| PS | 0.950 | 0.956 | 0.646 | 0.857 | 0.416 | ||
| IM | 0.927 | 0.941 | 0.695 | 0.642 | 0.478 | 0.757 | |
| VB | 0.953 | 0.962 | 0.809 | 0.761 | 0.195 | 0.694 | 0.734 |
Assessment of Structural Model
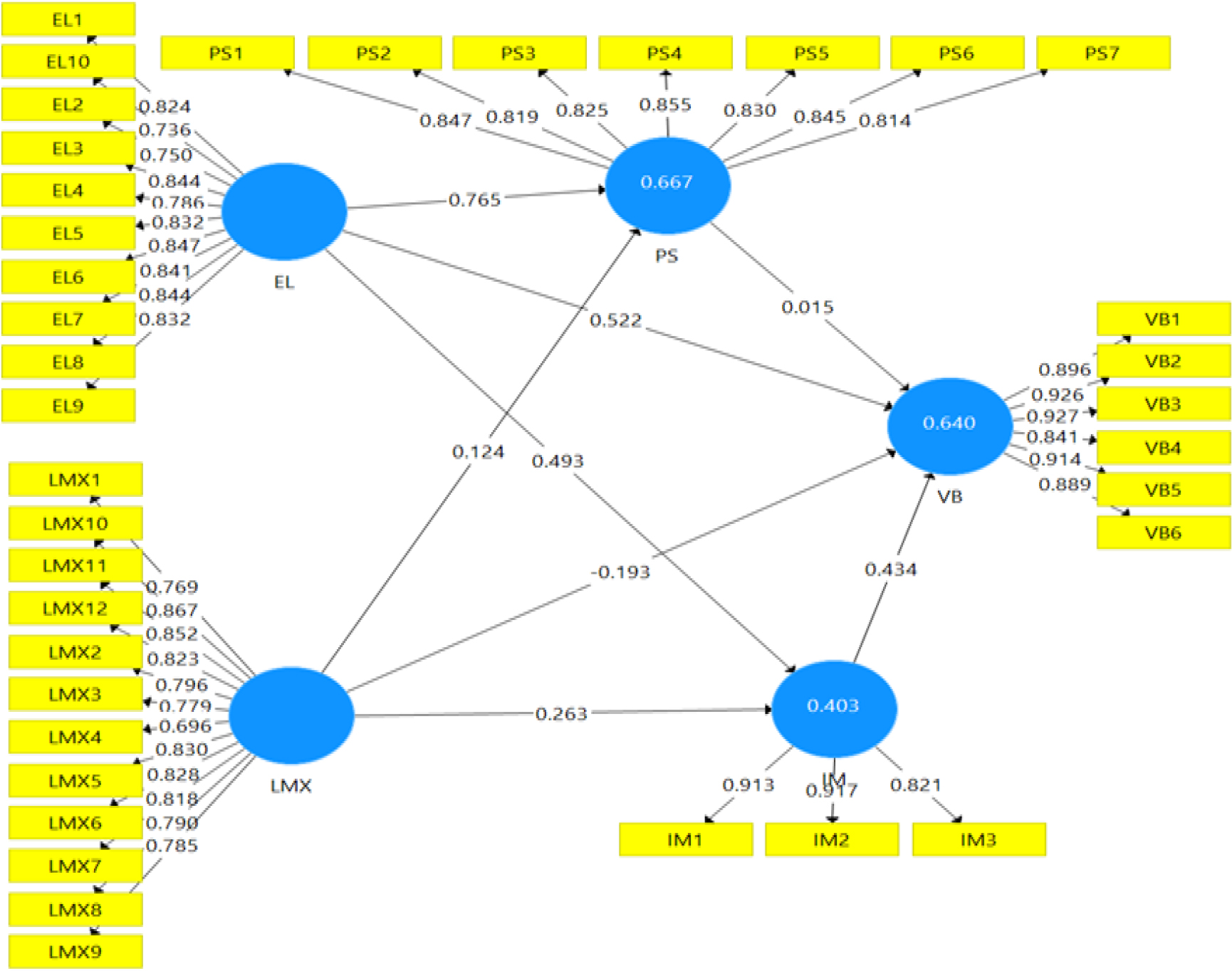
R-square values of endogenous latent variables are classified as robust (if R2 ≥0.75), moderate (if R2 ≥0.50 and <0.75), and weak (if R2 ≥0.25 and <0.50) following the recommendations of Hair et al. (2019); Hair Jr et al. (2017); Hair Jr et al. (2021). The model fit test results (see Table 3 and Figure 2) showed that El and LMX jointly contributed 66.7% and 40.4% variances in PS and IM, respectively. All the exogenous constructs explained 64.0% (R2 = 0.640) of the observed variance in VB. The analysis of effect size performed using the f-square value following the well-acknowledged guideline by Cohen (1988) guided the decisions: small effect (if f2 ≥0.02 and <0.15), medium effect (f2 ≥0.15 and <0.35) and substantial effect (if f2 ≥0.35). Following these references, only the PS construct did not affect the VB of nurses (f2 = 0.001). Other constructs’ effect sizes were between small and medium, as in Table 3. The Q-square values obtained through the blindfolding analysis using the SmartPLS 4 software indicated the direct and indirect models had good predictive relevance.
| Exogenous Construct | R-square Endogenous Construct | f-square effect size | Q-square Endogenous Construct |
|---|---|---|---|
| EL | Psychology Safety | 1.550 (large) | Psychology Safety |
| LMX | (0.667: Moderate) | 0.038 (small) | 0.458: Good predictive relevance |
| EL | Intrinsic Motivation | 0.359 (large) | Intrinsic Motivation |
| LMX | 0.102 (small) | (0.403: Moderate) | 0.310: Good predictive relevance |
| EL | Voice Behavior | 0.257 (medium) | Voice Behavior |
| LMX | 0.083 (small) | (0.640: Moderate) | 0.512: Good predictive relevance |
| PS | 0.001 (no effect) | ||
| IM | 0.264 (medium) |
Hypotheses Testing
The bootstrapping indirect effects are more robust in reporting mediation analysis (Hayes, 2017; Ramayah et al., 2018). Indeed, concerning Hayes, the bias-corrected bootstrap confidence interval is the most excellent approach for detecting mediating effects in scientific research. The indirect results obtained through the bootstrapping analysis with 5000 re-samples showed that the hypotheses (H2: β = 0.24, t-value = 7.116) and (H4: β = 0.114, t-value = 4.669) were significant. Furthermore, the indirect effects bias-corrected bootstrap at 95% confidence interval for (H2: BCLL = 0.160, BCUL= 0.279) and (H4: BCLL = 0.071, BCUL = 0.168) did not straddle a value of zero (0) in between, indicating there were mediations and it was statistically significant. In conclusion, the decision was that IM partially mediated relationships between the constructs EL-VB and LMX-VB. The first and third hypotheses (H1 and H3) were insignificant since the observed t-values were 0.300 and 0.285, respectively. Looking at the indirect effects’ bias-corrected bootstrap at 95% confidence interval for H1[BCLL = -0.090, BCUL = 0.110] and H3[BCLL = -0.014, BCUL = 0.020] found to straddle a value of ‘0’ in between the lower and upper values, giving an indication there were no mediation effects. As a final remark on the hypotheses testing, PS did not mediate the connection between (EL & VB) and (LMX & VB). The complete summary of the mediation analysis results is in Table 4.
| Hypotheses | Construct Relationship | Std. Beta (β) | σ | t-value | p-value | BCLL | BCUL | Decisions |
|---|---|---|---|---|---|---|---|---|
| H1 | EL> PS-> VB | 0.015 | 0.051 | 0.300 | 0.764 | -0.090 | 0.110 | Reject |
| H2 | EL -> IM -> VB | 0.214 | 0.030 | 7.116 | 0.001 | 0.160 | 0.279 | Accept |
| H3 | LMX -> PS->VB | 0.002 | 0.008 | 0.285 | 0.776 | -0.014 | 0.020 | Reject |
| H4 | LMX -> IM -> VB | 0.114 | 0.024 | 4.669 | 0.001 | 0.071 | 0.168 | Accept |
Note: bias-corrected bootstrap confidence interval for upper level (BCUL), bias-corrected bootstrap confidence interval for lower level (BCLL)
Discussions
Scholarly concern, debates, and critics about employee voice and behavior skyrocketed in the latter part of the twentieth century (Kim & Ishikawa, 2021; Maynes & Podsakoff, 2014). Misconducts can uncover through easy, casual talks that relate forward-thinking ideas. Studies have shown various voice behaviors discovered in multiple settings, from formal grievance processes to whistleblowing. Many academics consider the voice more than a reaction to harmful stimuli (Chen et al., 2018). In addition, various employees’ comfort levels are observable when bringing up concerns and providing feedback (Ilyas et al., 2021). However, the specific position of both constructs for mediators, psychological safety, and intrinsic motivation on the connections between empowering leadership and the impetus of leader-member exchange for nurses voicing behavior in public hospitals remains uncultivated mainly. Thus, an empirical study with a relevant nurse sample enables learning the associations and the research finding summarized in this paper to fill necessary gaps while encouraging continuous research. The research findings indicate that psychological safety cannot significantly mediate the nurses’ dynamic voice behavior and antecedents, namely empowering leadership and leader-member exchange, specifically in public hospitals.
Interestingly, it concurred that public hospitals help boost the nurses’ intrinsic motivation. This factor essentially worked as an intermediary on the research link between empowering leadership, LMX, and nurses’ voice behavior. Fairly treated workers are more likely to be productive and cooperative colleagues (Gigol, 2020). Employee exchange connection is positively related to feelings of emancipation, obligation, and increased internal dynamics of motivation to improve the surroundings directed toward the work ground (Bolino & Turnley, 2009; Chen et al., 2018; Duan et al., 2017; Lee et al., 2021). Psychological safety is frequently allied mainly with the constructs framed in this study, ‘empowering leadership’, ‘LMX’, and ‘voice behavior’. Employees are likelier to be happy and productive when they feel comfortable in their workplace and can express themselves openly and without fear of repercussions (Edmondson & Lei, 2014; Maynes & Podsakoff, 2014). However, we found that psychological safety seems to remain intrinsic and is not the primary concern of the nurses during the engagement with voice behaviors. Indeed, a public hospital with a good governance structure overrides the role of psychological safety compared with intrinsic motivation. Ensuring work stability during high volatility and uncertainty makes the nurses feel secure. In turn, the empirical evidence in this paper shows that it may encourage nurses to speak up.
Furthermore, leaders with profound leadership behavior increased nurses’ intrinsic motivation and concurrently built up nurses’ voice behavior. Nurses’ innate drive helps develop interpersonal competence and inherent appeal that does not depend on tangible rewards. Nurses with professional nursing practice have proven to handle difficult situations, akin to the expressive note of Lyman et al. (2020) and Kee et al. (2021). Also, Malaysian public hospital nurses can speak up due to their knowledge, practice experience, work culture, and supportive leaders who believe in engaging nurses in every spear of innovative strategies. Tenancy grows in nurses’ roles over time, which may support their tendency to become more vocal in the workplace. Leaders’ inclusiveness and equality practices increase nurses’ voice behavior, and perhaps to Hanson et al. (2020), the reverse will delimit voice behavior among nurses at any stage in the organizational structure. Since their employer has shown a willingness to care for their well-being, nurses participating in the reciprocation process are firmly in anticipation to actively partake in hospital, work, and society-related actions. These moves could stimulate and grow the hospital’s innovative work-based behavior dedicated to sustainable performance (Ilyas et al., 2021; Jada & Mukhopadhyay, 2019; Jung et al., 2020; Svendsen et al., 2018).
Nurses’ accumulated pleasant experiences and enhanced learning curves lead to a robust internal-external professional network, innovation, competencies, and profound provision of hospital services. Nursing professionals may be reluctant to raise concerns about unprofessional behavior or other areas where a value judgment implies fear of repercussions from superiors or coworkers (Gigol, 2020; Martinez et al., 2015). But, in the Malaysian context, this situation is curbed and is not an issue to be concerned about since the findings indicate that psychological safety does not rule out the strength of the voices. This study proves that for nurses who genuinely believe their voices are valued and translated into actions, redundancy in further voice actions will follow with the conjoin of intrinsic motivation.
Due to advancements in the hospital service revolutions, breaking the status quo has become necessary; thus, the nurses’ fraternity is undoubtedly the supporting milieu for service victory. Indeed, the study’s findings encourage the growing knowledge of how leadership, intrinsic motivation, and psychological safety may affect nurses’ willingness to speak up, particularly in the public sector. With certain limitations, it is possible to capture the ideas presented in this research and apply them to private healthcare providers, hospitals, or any related field. The SET and LMX theories are utilized and supported throughout this research. However, some researchers find that SET favors positive reciprocity, while others find it detrimental (Cropanzano et al., 2017; Cropanzano et al., 2003).
Limitations and Recommendations for Future Research
The instrument’s reliability and validity are satisfactory. However, because the research focused on public hospitals, the study may have some flaws, and further research is needed to determine if or not other characteristics are just as important. Nevertheless, the research methods employed herein are valuable for application in a wide range of future studies, both in and out of the business world. The research approach is supposed to inspire academics, which will contribute to expanding our understanding of how employees in various work environments use their voices. Exploring the differences between employees’ formal and informal voice behaviors would be a great addition to future research.
Implications of the Study to Nursing Practice
Nursing is carried out methodically by following a deliberate, logical, and reasonable approach to problem-solving. From the initial assessment through the final review, the nursing process incorporates ongoing input from the patients, peers, their families, their communities, and other professionals’ connectivity. At this juncture, nurse voice behavior is a duty in executing responsibilities as imposed in this study. Nursing requires specific professional endorsement and registration or licensing by the authority. It is a trust given to a particular group of people passionate about caring behavior. Experiences gained via direct and indirect involvement in patient care, administrative work, education, training, research, consultation, mentoring, and coaching mold nurses into more conscious individuals. Their intellectual maturity encourages them to be more vocal for the betterment of humanity. Thus, competencies to engage in voice behavior while understanding the antecedents, potential limitations, and constructive remedies help the nursing fraternity be evergreen in making a difference and becoming change agents with the power of talk. The outcomes of this research are straightforward: intrinsic motivation encourages and surpasses psychological safety to express voice behavior. Utterly passionate about the core values of nursing practice, voice behavior advanced for its inherent satisfaction, challenges entailed tangible receivable such as rewards instead. At the peak of demonstrating the voice behavior, empowering leadership is necessary, then having a leader-member exchange governing. Those leading the nursing practice by all means challenged to change the conventional to empowering leadership style.
Conclusion
Understanding the practices, power, dysfunction, and prohibitions of voice behavior from time to time in the hospital setting is crucial for the hospital management and stakeholders such as patients, NGOs, volunteers, nurses, etc. The study finding paths several ideas for nurse managers and other leaders to support voice behavior while strengthening psychological safety and intrinsic motivation, demonstrating vital points for nurses to become more willing to speak up. Continuous professional nursing orientations, training, seminar, workshops, and alike provides an opportunity for enhancing proper voice behavior with the responsibilities of their role. Enhancing peer learning and establishing a knowledge management portal helps spread innovative thought, gain knowledge, and build self-confidence, improving voice behavior that enhances performances. Adding an encouraging culture of mentor-mentee will dynamically boost self-leadership qualities among nurses that entail positive voice behavior. Mentors (senior-junior partnership) can act as an informal, immediate point of expert reference to make nurses (mentees) feel more peaceful and vital to the job, increasing their chances of actively speaking up. Policy, procedures, and guidelines that officially permit open dialogue and inquiry must be transparent for everyone to gauge and embrace in their daily work routine. These can help overcome the feeling of insecurities nurses may experience at the beginning of their careers till the end. Although significant labor hours are needed in planning, organizing, leading, and strategically implementing changes, the outcomes are worth it for the nation. More competent nurses will advance work culture, provide excellent healthcare services and manage publicly funded hospitals with overarching trust.