









Background
Cancer presents a major crisis for the patients and their family caregivers. Cancer often requires hospitalization, regular follow-up, and repeated care in the hospital or at home (Sung et al., 2021). At some points, especially during the latter stage, patients with cancer receive palliative care. Palliative care is an approach to enhancing the quality of life of both the patients and the family caregivers (World Health Organization (WHO), 2020). Family involvement is profound for optimizing treatment and ensuring medication adherence, guaranteeing the continuity of care, and providing social support for the patient. Unlike High-Income Countries (HICs), where formal support is mostly available, the burden of cancer in Low-Income Countries (LICs) is significant due to the help-seeking behavior and delays of cancer care, which are common in the regions (Brand et al., 2019; McCutchan et al., 2021; Petrova et al., 2022).
No one is ready to become a family caregiver (Kristanti et al., 2021), and family members need support and facilitation to prepare themselves for this role. During caregiving, caregivers often feel that their own needs are often overlooked (Tarberg et al., 2019); they embody multiple roles, such as being a breadwinner, a person in charge of care continuity, and a suffering minimizer as well as contributors in the decision-making process (Reigada et al., 2015). Family caregivers often feel a lack of readiness and heavy burdens, leading to depression and a decrease in their overall quality of life. As a result, many of them rate their quality of life as fair or poor (Williams, 2018). Therefore, healthcare professionals can play a crucial role in facilitating and guiding these family caregivers during this challenging period.
As part of a multidisciplinary team, nurses play a significant and unique role in palliative care. Their involvement is not limited to the late stages of the disease; they also facilitate patients’ wishes and values while easing discussions during advance care planning (Fliedner et al., 2021). In palliative care, nurses’ roles are mostly assessed on how they care for patients, support family caregivers, and meet professional requirements (Soikkeli Jalonen et al., 2020). Although the evidence is still limited, a previous study showed that nurses-led interventions in palliative care in Low- and Middle-Income Countries (LMICs) appear promising and feasible to be conducted (Bassah et al., 2023).
There are existing gaps in palliative care development between HICs and LICs. First, palliative care services are mostly available in the HICs. The level of palliative care globally has been mapped using indicators such as palliative care coverage, public awareness, education and training, and the availability of opioids (Lynch et al., 2013). Other mapping used indicators such as palliative care health care environment, human resources, affordability and quality of care, and community engagement (The Economist Intelligence Unit, 2015). Both mappings have shown that the LICs are mostly ranked lower (Lynch et al., 2013; The Economist Intelligence Unit, 2015). This indicates a scarcity of formal care and support for patients in need of palliative care services. Second, due to the limited number and quality of healthcare professional support in LICs, patients heavily rely on support from their family and relatives (Abdel-Malek et al., 2019; Lambert et al., 2017) for practical assistance, such as medication management and feeding (Kristanti et al., 2017) as well as for the decision-making process (Kusi et al., 2020).
Additionally, most patients needing palliative care in LICs prefer to stay home (Zhu et al., 2021). Consequently, family caregivers in this region bear a significant burden without adequate support, facing physical, psychological, and financial challenges that are often only partially addressed by relatives and friends (Thrush & Hyder, 2014). Thirdly, in most LICs, a strong culture of familism and caregiving is passed down from generation to generation. Therefore, caregiving is pivotal and seen as an essential act of service to show respect to elders (Kristanti et al., 2019). Families tend to take an active role in providing personal care (Ho et al., 2021) and give longer hours for caregiving even during hospitalization (Hogan et al., 2022). Due to the lack of resources, family caregivers in LICs manage severe complications with limited health knowledge and little professional healthcare input (Ho et al., 2021). As a result, education for family caregivers in LIC settings may be more complex than in HICs.
Providing educational intervention is a global research and development agenda that aims to address the instructional needs of family caregivers to effectively provide care at home (Hasson et al., 2020). Some review studies have shown that family caregivers acknowledged that education is significantly needed throughout the disease trajectory (Flemming et al., 2019; Kusi et al., 2020). Information related to patient care, such as symptom management, will be much appreciated by family caregivers since patients with cancer most likely suffer from many symptoms (Zhu et al., 2021). However, previous research reported that more than half of family caregivers had never heard of palliative care terminology, and only around 19.2% knew and could explain it to others (Dionne Odom et al., 2019).
Previous reviews have been conducted to explore interventions that support family caregivers (Ahn et al., 2020; Hudson et al., 2010; Li et al., 2021), including educational interventions (Bilgin & Ozdemir, 2022; Phongtankuel et al., 2018; Reigada et al., 2014). However, these reviews revealed that the majority of evidence was retrieved from HICs, highlighting the need for diversity in information from various ethical, cultural, and economic backgrounds (Ahn et al., 2020; Hudson et al., 2010; Li et al., 2021). Considering the complexity of the need for education for family caregivers in LICs, it is essential to identify the gaps in education support available in this region—reflection on the evidence from HICs, where palliative care services are well-established and can offer valuable insights. Therefore, the current review aims to identify and compare the existing implementation of education for family caregivers of patients with advanced cancer in LICs and HICs.
Methods
An integrative review study was employed using a guideline developed by Whittemore and Knafl (2005). The review was conducted following six steps, namely: 1) identification of problems and objectives, 2) determining the literature search strategy, 3) data selection, 4) data evaluation, 5) data analysis, and 6) data presentation.
Identification of Problems and Objectives
In the current review, we categorized the problems into several subsequent interests: the concept, target population, and healthcare problem (Whittemore & Knafl, 2005). The concept was an education or training program given to family caregivers. The target population and health care problems were articles related to family caregivers of patients with cancer. The main objective of this review was to explore the education provided to family caregivers of cancer patients in both HICs and LICs.
Determining the Literature Search Strategy
Our literature search and selection strategy used the following databases: PubMed, EBSCO, ProQuest, and ClinicalKey. The keywords used were ‘family caregiver AND education OR training AND palliative care AND cancer’. Detailed information on the search method is presented in Table 1.
| Database | Keywords/Search Queries | Filter | Results | Update |
|---|---|---|---|---|
| PubMed | ((((family caregiver[Title/Abstract]) AND (education[Title/Abstract])) OR (training[Title/Abstract])) AND (palliative care[Title/Abstract])) AND (cancer[Title/Abstract]) AND (clinicaltrial[Filter] OR randomizedcontrolledtrial[Filter]) | Clinical trial RCT | 50 | 14 |
| EBSCO | AB family caregivers AND AB ( education or training ) AND AB ( palliative care or cancer ) | English language | 93 | 32 |
| ProQuest | title(family caregiver) AND title(education) OR title(training) AND title(palliative care) AND title(cancer) | English language Document type: article | 15 | 4 |
| ClinicalKey | family caregiver AND education OR training AND palliative care AND cancer | RCT Meta-analysis | 21 | 0 |
| Total | 179 | 50 |
Result: searched on 18 November 2021 | Update: searched on 8-9 August 2023
Two independent reviewers (M and NWH) conducted an initial screening of titles and abstracts to identify eligible articles. The following inclusion criteria were written in English, focusing on palliative care education or training for family caregivers and adult cancer patients. The search was conducted on 18 November 2021 and updated on 8-9 August 2023 (See supplementary file). Papers were excluded if they focused on informal caregivers with no blood relation and involved financial consequences in providing care or pertained to non-cancer populations. Papers that were mainly providing educational training for patients would also be excluded. Review papers were also excluded.
After the abstract and title screening, the authors independently examined the full-text articles to determine the eligibility of the articles. In cases of discrepancies, especially during the paper selection process, all authors met and discussed them until a consensus was reached.
Data Selection
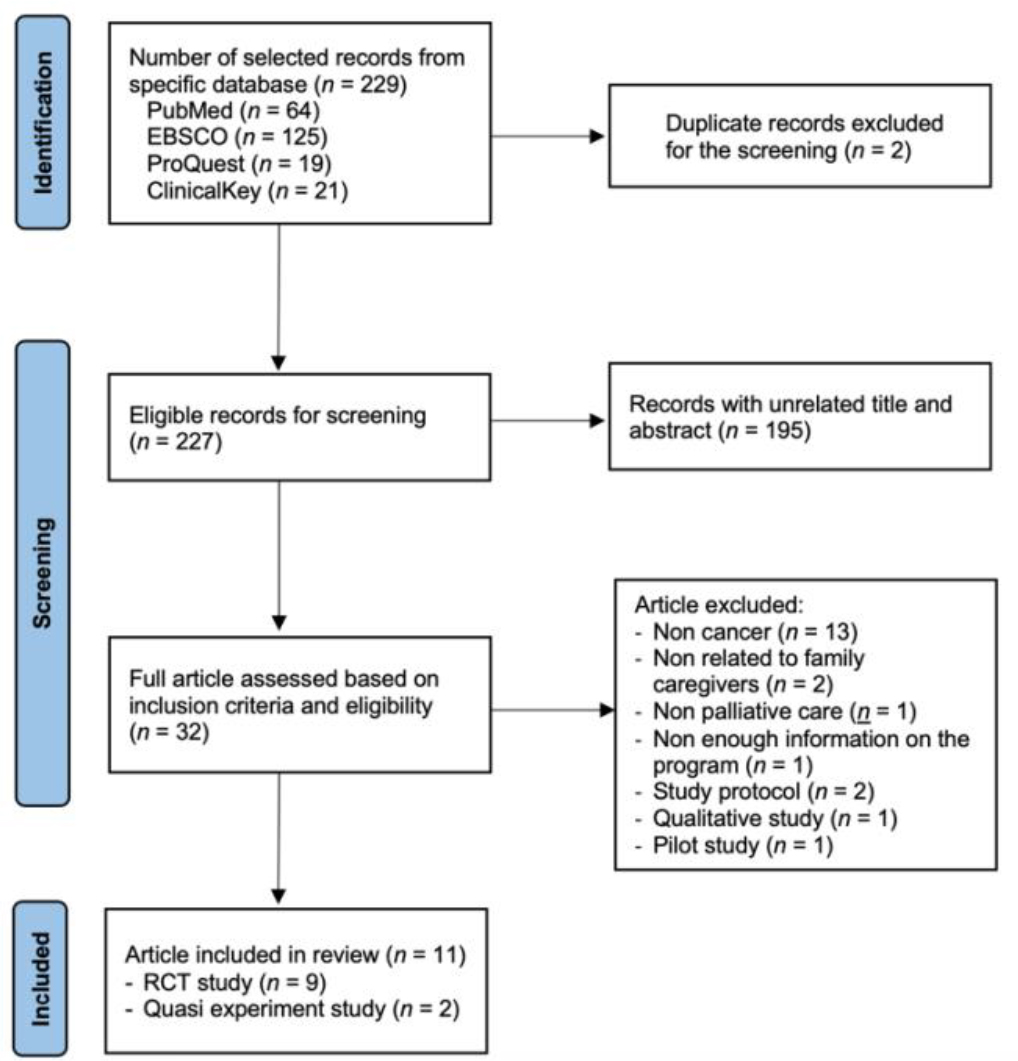
Our initial search yielded 229 studies. After removing two studies due to duplication, 227 were screened for title and abstract. Thirty-two studies met our criteria for a full-text review, and 21 were excluded for several reasons, such as not addressing cancer, not focusing on family caregivers, not addressing palliative care, no description of the education used, protocol study, qualitative and pilot study. Finally, eleven studies were used in the review (Figure 1. Preferred Reporting Items for Systematic Reviews and Mata-Analyses (PRISMA) flow chart for selection of the studies) (Moher et al., 2009).
Data Evaluation
The articles were evaluated using critical appraisal tools from the Joanne Briggs Institute (JBI) (Joanna Briggs Institute, 2017). Two authors independently assessed the studies. When there were disagreements, all authors discussed until a consensus was reached. Scoring was not used to exclude papers. The main aim of this evaluation is to get the answer on how well a study was designed and performed to avoid bias (Munn et al., 2023). RCT and quasi-experiment appraisal tools were used based on the study design used by the research article. For the JBI tools, responses were recorded as ‘yes’ if information was found, ‘no’ if a particular item was not conducted, ‘unclear’ if there was uncertainty, and ‘not applicable’ if it did not relate to the study being evaluated (Munn et al., 2014). The quality of each included article was categorized as low (less than 65%), moderate (65-85%), or high (80%) (Negash et al., 2023). In the current review, nine papers were ranked moderate, and two were rated high quality (Table 2). Involving a sufficient quality paper will maintain the quality of a review paper (Munn et al., 2023).
| No | Author (Year) | JBI Form | Yes | No | Unclear |
|---|---|---|---|---|---|
| 1 | Belgacem et al. (2013) | RCT Appraisal Tool | 69% | 31% | - |
| 2 | Holm et al. (2016) | RCT Appraisal Tool | 69% | 31% | - |
| 3 | Hudson et al. (2015) | RCT Appraisal Tool | 77% | 15% | 8% |
| 4 | Hudson, Aranda, and Hayman-White (2005) | RCT Appraisal Tool | 69% | 31% | - |
| 5 | Kizza and Muliira (2019) | Quasi-Experimental Appraisal Tool | 89% | 11% | - |
| 6 | Kristanti, Setiyarini, and Effendy (2017) | Quasi-Experimental Appraisal Tool | 78% | 11% | 11% |
| 7 | Narayanan et al. (2023) | RCT Appraisal Tool | 85% | - | 15% |
| 8 | Schulman-Green et al. (2023) | RCT Appraisal Tool | 77% | - | 23% |
| 9 | Shohani et al. (2018) | RCT Appraisal Tool | 62% | - | 38% |
| 10 | Li, Ling, and Zhanyu (2019) | RCT Appraisal Tool | 77% | 15% | 8% |
| 11 | Yanwei et al. (2018) | RCT Appraisal Tool | 69% | 31% | - |
Data Analysis
We followed the integrative review guideline developed by Whittemore and Knafl (2005) to conduct data analysis, which involved several steps: data reduction, data comparison, conclusion drawing, and data verification. The first step was data reduction. Important information related to the objectives of the current review was extracted from studies that met the inclusion criteria. Data were extracted using a form that consists of: 1) study characteristics: purpose, design, year, origin of study; 2) sample characteristics: age, diagnosis, data source; and 3) education/training: topic, duration, frequency, media, and education provider.
The second step was data comparison. Data were compared and contrasted in this stage to identify patterns, themes, or essential relationships among concepts (Whittemore & Knafl, 2005). Data extracted in the previous stage were repeatedly compared across sources to highlight important information. In this step, data were grouped by country’s income according to World Bank Income Levels. From the six classifications, we further classified countries into two: HICs, which consist of high-income, upper-middle-income countries, and LICs, which consist of middle-income, low and middle-income, lower-middle income, and low-income countries. The next step was the conclusion drawing and data verification. Each extracted data item was compared across studies, and similar data were grouped as categories for further analysis and synthesis. Throughout the analysis, we used a matrix to provide more information on the implementation of education programs for family caregivers of patients with cancer in HICs and LICs. This was conducted iteratively until a consensus was reached. Finally, data were presented in tables to describe the included papers and tables for presenting data synthesis for education and training for family caregivers in HICs and LICs.
Results
Eleven studies were used in the current review. Therefore, they were compiled during data synthesis.
Characteristics of the Included Studies
Out of the eleven studies, seven were from HICs, namely Australia (Hudson et al., 2015; Hudson et al., 2005), America (Schulman-Green et al., 2023), China (Li et al., 2019; Yanwei et al., 2018), France (Belgacem et al., 2013) and Sweden (Holm et al., 2016). Meanwhile, four studies were from LICs, namely India (Narayanan et al., 2023), Indonesia (Kristanti et al., 2017), Uganda (Kizza & Muliira, 2019) and Iran (Shohani et al., 2018). All studies from HICs used RCT, and the two studies that used quasi-experiments were from LICs (Table 3).
| Author (Year) | Intervention / Given to / Theoretical Framework (TF) | Content and Healthcare professionals involved | Procedure | Media / Mode of delivery / Duration / Frequency | Main outcome |
|---|---|---|---|---|---|
| Belgacem et al. (2013) RCT France (HIC) |
|
|
|
|
Quality of life of patients and Carers as well as Burden of Carers |
| Holm et al. (2016) RCT Sweden (HIC) |
|
Promote preparedness to be caregivers:
|
|
|
Preparedness for caregiving |
| Hudson et al. (2015) RCT Australia (HIC) |
|
Promoting psychological well-beingHealthcare professionals involved: Nurse | Two education programs: home visits and phone calls
|
|
Psychological distress |
| Hudson, Aranda, and Hayman-White (2005) RCT Australia (HIC) |
|
Psychoeducational intervention:
|
|
|
Readiness of family caregiver |
| Kizza and Muliira (2019) Quasi experiment Uganda (LIC) |
|
Cancer pain management Healthcare professionals involve: Nurses and peer support volunteer (PSV) |
|
|
Pain knowledge and pain management |
| Kristanti, Setiyarini, and Effendy (2017) Quasi experiment Indonesia (LIC) |
|
Basic care training for family caregivers in how to complete personal hygiene for patients with cancer in a bedridden position Healthcare professionals involved: Nurse |
|
|
Quality of life family caregiver |
| Narayanan et al. (2023) RCT India (LIC) |
|
|
Intervention group watched a video. After that, they were instructed to implement it at home |
|
Quality of life of patients and family caregivers |
| Schulman-Green et al. (2023) RCT USA (HIC) |
|
|
|
|
Palliative care literacy |
| Shohani et al. (2018) RCT Iran (LIC) |
|
|
|
|
Quality of care for family caregivers |
| Li, Ling, and Zhanyu (2019); Yanwei et al. (2018) RCT China (HIC) |
|
|
The sessions were conducted on 3 different days each week during treatment by a multidisciplinary team |
|
Quality of life and psychological variables for patients with non–small cell lung cancer stadium III and IV |
Characteristics of Education Programs in HICs and LICs
In the HICs, training programs for family caregivers were about psycho-education (Holm et al., 2016; Hudson et al., 2015; Hudson et al., 2005), wellness education (Li et al., 2019; Yanwei et al., 2018), managing cancer care using caregivers’ guides (Schulman-Green et al., 2023), and providing nursing care to patients (Belgacem et al., 2013). Meanwhile, in the LICs, training programs were about basic care training for caregivers (Kristanti et al., 2017), pain management (Kizza & Muliira, 2019), palliative care training (Shohani et al., 2018), and education programs using video (Narayanan et al., 2023). Only four studies (Holm et al., 2016; Hudson et al., 2015; Hudson et al., 2005; Schulman-Green et al., 2023), all from HICs, utilized a theoretical framework to develop their educational programs.
Apart from three studies that did not mention the education tool (Holm et al., 2016; Li et al., 2019; Yanwei et al., 2018), the majority of programs used modules as educational tools (Hudson et al., 2005; Kizza & Muliira, 2019; Kristanti et al., 2017; Schulman-Green et al., 2023). One study used only video (Narayanan et al., 2023). Two studies combined modules with video (Kristanti et al., 2017) and audio (Hudson et al., 2015). Some studies used leaflets (Belgacem et al., 2013) and booklets (Shohani et al., 2018).
All programs lasted between three weeks (Holm et al., 2016; Narayanan et al., 2023), four weeks (Hudson et al., 2015; Hudson et al., 2005; Kristanti et al., 2017), five weeks (Belgacem et al., 2013), eight weeks (Schulman-Green et al., 2023; Yanwei et al., 2018) and 12 weeks (Kizza & Muliira, 2019; Shohani et al., 2018). The average duration is between 15 and 60 minutes. Most programs involved home visits, while two programs were combined with tele-nursing (Shohani et al., 2018) or phone calls (Hudson et al., 2015) in order to tackle geographical challenges.
More professions were involved in the palliative care education for family caregivers in HICs than in LICs. Studies in HICs, namely China (Li et al., 2019; Yanwei et al., 2018) and Sweden (Holm et al., 2016) involved multidisciplinary teams. Two programs in LICs involved only nurses, one study in Uganda involved volunteers, and a study from India involved a multidisciplinary team (Narayanan et al., 2023).
Comparison of Education Programs Between HICs and LICs
We classified programs into four aspects: physical, psychological, social, and spiritual. In total, there were 18 topics: nine were related to physical aspects, six were related to psychological aspects, two were related to social, and one was related to spiritual aspects. Three studies (Kizza & Muliira, 2019; Li et al., 2019; Narayanan et al., 2023; Yanwei et al., 2018) provided intervention for patients and family caregivers, while the other studies were given only to the family caregivers.
As shown in Table 4, psychological well-being was the most common topic for palliative care education for family caregivers, as it was reported in three HICs studies (Holm et al., 2016; Hudson et al., 2015; Hudson et al., 2005) and one study in LIC (Shohani et al., 2018). No studies were found in LICs providing educational programs related to social and spiritual aspects for the family caregivers.
| Topics | HICs | LICs | |||||||||
|---|---|---|---|---|---|---|---|---|---|---|---|
| Belgacem et al. (2013) | Holm et al. (2016) | Hudson et al. (2015) | Hudson, Aranda, and Hayman-White (2005) | Li, Ling, and Zhanyu (2019); Yanwei et al. (2018) | Schulman-Green et al. (2023) | Kizza and Muliira (2019) | Kristanti, Setiyarini, and Effendy (2017) | Shohani et al. (2018) | Narayanan et al. (2023) | Total | |
| Physical | |||||||||||
| Pain management | √ | √ | √ | 3 | |||||||
| Activity Daily Living (ADL) | √ | √ | √ | √ | 4 | ||||||
| Physical therapy | √ | √ | 2 | ||||||||
| Physical activities | √ | √ | 2 | ||||||||
| Nutrition | √ | √ | √ | √ | 4 | ||||||
| Symptom management | √ | √ | √ | √ | 4 | ||||||
| Complication of chemotherapy | √ | 1 | |||||||||
| Cancer and palliative care concept | √ | √ | √ | 3 | |||||||
| Wound care | √ | 1 | |||||||||
| Psychological | |||||||||||
| Psychological well-being | √ | √ | √ | √ | 4 | ||||||
| Body image and self-confidence | √ | √ | 2 | ||||||||
| Roles and needs of family caregivers | √ | √ | √ | 3 | |||||||
| Bereavement preparation | √ | √ | 2 | ||||||||
| Coping strategies | √ | √ | 2 | ||||||||
| Self-care for family caregivers | √ | 1 | |||||||||
| Social | |||||||||||
| Social needs | √ | 1 | |||||||||
| Communication | √ | 1 | |||||||||
| Spiritual | |||||||||||
| Spirituality | √ | √ | 2 | ||||||||
Discussion
The current review aimed to identify and compare the existing implementation of education for family caregivers in LICs and HICs. We found that psychological well-being was the most common topic for both regions. Limited studies in LICs focused on social and spirituality for palliative care education for family caregivers. Various healthcare professionals were involved in the HICs, while in LICs, most intervention programs were facilitated by nurses.
Education for Family Caregivers in HICs and LICs
Providing information through training and educational programs for family caregivers is essential in reducing confusion and preparing them for their caregiving roles (Bilgin & Ozdemir, 2022). A proper training or education program given to family caregivers can significantly increase their comfort with caregiving roles, assist with closure, and gain caregivers’ confidence (Kwak et al., 2007). However, there is a limitation in publications concerning education for family caregivers, suggesting that there may be limited findings to support such studies (Reigada et al., 2014). Previous reviews indicate that demographic characteristics, particularly gender, play a significant role in determining the most appropriate setting for educational programs. Women, in particular, are considered ideal carers (Bilgin & Ozdemir, 2022), and therefore, women are mostly the target persons to receive educational programs.
The current review has shown that studies in HICs have covered important aspects of palliative care education for family caregivers: physical, psychological, social, and spiritual. Meanwhile, studies in LICs have involved topics on the physical and psychological aspects but are still lacking in social and spiritual aspects. There are at least two explanations. First, the lack of topics on social and spiritual aspects is related to the lack of resources. Data in the current review revealed that in LICs, all education interventions were guided by nurses. Therefore, the programs focused on physical and psychological aspects only. Secondly, since those aspects were embraced in everyday life, the LICs might not see the urgency for including social and spiritual topics. For example, in Indonesia, the spiritual aspect is part of identity. It becomes an essential part of everyday life (Rochmawati et al., 2018), including during caregiving activity (Kristanti et al., 2019). However, we believe that this area needs to be further explored.
Psychological Well-Being as the Most Common Topic for Palliative Care Education for Family Caregivers in HICs and LICs
Previous reviews have shown that psychological burden is the most frequently reported problem in LICs (Kusi et al., 2020) and in some studies in HICs (HICs) (Chua et al., 2020; Morales Aliaga et al., 2021). This burden can be attributed to the patient’s condition and the assumptions surrounding the caregiver’s roles (Kusi et al., 2020). Data from the current review has shown that topics for supporting psychological well-being in HICs were more varied than in LICs. Also, no study from LICs covered issues of bereavement, self-care, and coping strategies for family caregivers. Psychological well-being is a crucial aspect of palliative care, and it may require a longer period to enhance caregivers’ well-being. A previous study mentioned that educational programs may significantly improve short-term performance, such as caregivers’ preparation and self-efficacy, but may not immediately impact psychological well-being (Hendrix et al., 2016).
Theoretical Framework to Develop an Intervention
We observed only four in the current review (Holm et al., 2016; Hudson et al., 2015; Hudson et al., 2005; Schulman-Green et al., 2023). Out of eleven articles, theoretical frameworks were used for interventions. Utilizing theories for interventional programs is essential to capture the complexity of the topic being studied and to provide conceptual thinking and program design (Davidoff et al., 2015). It is crucial not only to apply popular theories but also to consider the applications of developing theories. Researchers should clearly understand how the problem under consideration is related to the context in which it is applied (Moore & Evans, 2017).
Focus of Palliative Care Education
In the current review, we aimed to examine whether the education provided for family caregivers would primarily benefit the patients or offer advantages for the family caregivers themselves. The results demonstrated that the interventions could provide equal benefits for both parties. It was observed that the educational interventions given to family caregivers predominantly focused on providing information to enhance their ability to care for the patients rather than prioritizing their own well-being (Kristanti et al., 2023).
Multidisciplinary Team
Our review found that studies in HICs involved more healthcare professionals in education for family caregivers, while in LICs, it is mostly facilitated by nurses (3 out of 4 studies). This aligns with previous research, which mentioned that in LICs, interventions were commonly led by nurses since nursing is a profession that is most often involved in various interventions in palliative care compared to other healthcare providers (Phongtankuel et al., 2018). One recent systematic review has shown that nurse-led interventions are more effective than multidisciplinary ones (Bilgin & Ozdemir, 2022). This may be due to the complicated communication that often happens within multidisciplinary work. Apart from its challenges, multidisciplinary teamwork for palliative care is still considered essential to increase social well-being and lower psychological distress and caregiver burden compared to those who received the usual care (Sun et al., 2015). The WHO asserted that palliative care service consists of at least physicians, nurses, social workers, and volunteers (World Health Organization (WHO), 2020). The most common issue in LICs is the limited number of healthcare professionals in oncologic care (Shah et al., 2019). This shortage may limit their focus to only the patients’ needs (Shah et al., 2019) and overlook the needs of the family caregivers.
The Use of Media during Education Programs for Family Caregivers
There are a few differences in the media used for palliative care education in HICs and LICs, both of which utilize print media (booklets, leaflets, etc.) and audiovisual materials. The selection of media is crucial in training programs (Agarwal & Epstein, 2017) and should be based on the learning needs of the learners and the availability of media resources. Video interventions have been proven useful for experimental studies involving patients and family caregivers in palliative care (Cruz Oliver et al., 2020).
Implications for Nursing Practice
Our review has described that education interventions for family caregivers, especially in LICs, were mostly initiated by nurses. This implies that sufficient competency is essential for nurses in palliative care settings. The recent systematic review has identified six competencies for palliative care nurses: leadership, communication, collaboration, clinical experiences, ethic-legal, psycho-social, and spiritual competencies (Hökkä et al., 2020). A lack of competencies will limit nurses’ involvement in supporting end-of-life discussions with patients and their family caregivers (Ikander et al., 2022). Regarding nurses’ role in providing intervention, a recent review revealed that nurses are involved in activities such as needs assessment, psychoeducation, practical support with caregiving, and peer support (Becqué et al., 2019). These nursing interventions have a positive effect on the preparedness, competence, rewards, and burden of family caregivers (Becqué et al., 2019). A recent review revealed that palliative care education mostly targeted healthcare professionals (Li et al., 2021). This indicates that there is an urgent need for nurses to contribute to the development of education interventions for family caregivers.
Conclusion
The current review compared and contrasted education interventions in HICs and LICs. We found variations in the implementation of palliative care education topics in these regions while also identifying some similarities. Both regions emphasize the importance of addressing the psychological needs of family caregivers. However, in LICs, the social and spiritual aspects of family caregivers were found to be lacking. Future studies should explore the need for assessment for education interventions in this region to determine if the lack is due to caregivers’ preferences or simply resource limitations. Moreover, healthcare professionals in LICs should urgently establish education interventions that would be appreciated by patients and family caregivers. While the current review identified various topics, it did not delve into the depth of education interventions for both regions. This aspect would be interesting to explore in future studies, as both regions can learn from each other’s experiences and practices.