










Background
Worldwide, the rates of smoking among men and women show a considerable contrast, with women’s rates projected to decrease to 6.6% by 2025, whereas men’s smoking rates remain high at 34.3% (World Health Organization, 2023). The smoking rate in Thailand is 41.3% among men, which is higher than the global rate while only 2.9% among women (World Health Organization, 2021), indicating that more women are still exposed to harmful substances from tobacco smoke even though they do not smoke. Passive smoking refers to the involuntary inhalation of smoke from cigarettes or other tobacco products smoked by other people, which can also include second and third-hand smoking (SHS and THS) (Eldridge, 2023). The rate of SHS exposure at home surveyed from women in 57 low- and middle-income countries was 24.4%, which was higher among pregnant women than non-pregnant women (Yang et al., 2022). In Thailand, the rates were higher at 55.4% (Jantarasiew et al., 2021) and 57.2% (Sonthon & Sonthon, 2019). These statistics show that passive smoking is highly prevalent and a significant concern, especially among pregnant women, which can cause various adverse pregnancy outcomes.
Tobacco smoke consists of more than 7,000 chemicals, including hundreds that are toxic (Centers for Disease Control and Prevention, 2022a). In pregnancy, the substances, particularly carbon monoxide, tar, cadmium, and nicotine (McDonnell & Regan, 2019), formaldehyde, and nitrogen oxides (Bernardini et al., 2022) in tobacco smoke harm the fetus (McDonnell & Regan, 2019). Various adverse fetal outcomes include low birth weight (Bernardini et al., 2022), congenital anomalies (Zhao et al., 2020), mental and behavioral problems (Tongmuangtunyatep et al., 2019), cardiovascular diseases, cancer, respiratory tract diseases, and metabolic diseases (World Health Organization, 2023). Therefore, prevention of pregnant women from prenatal passive smoking, especially at home, is crucial for nurses and healthcare professionals.
Pregnancy is theorized as the best moment for women to deal with their husbands’ smoking since their perception of health risks for their babies is heightened. Furthermore, women can substantially access health information and services during pregnancy. Unfortunately, prenatal services in Thailand lack comprehensive interventions and health education regarding passive smoking. This gap exists due to insufficient practical knowledge and limited studies involving pregnant women in the Thai context.
While one study identified social support and perceived barriers as predictors of preventive behavior against cigarette smoke exposure among Thai pregnant women (Pookpan et al., 2021), it did not explore factors related to husband-wife interactions. Another study found that permission for smoking at home was associated with secondhand smoke (SHS) exposure during pregnancy (Sonthon & Sonthon, 2019). However, establishing a smoke-free home was among the least practiced preventive behaviors against SHS exposure among Thai pregnant women (Jantarasiew et al., 2021). A community-based survey revealed community members’ support for smoke-free homes. This could be achieved by establishing a community agenda that involves participation and coordination among community members, family members, and current smokers (Suteerangkul et al., 2019).
Based on the experiences of Thai smoking men, their concern for their pregnant wives, particularly those with anemia, led to attempts to quit smoking. Despite their efforts, they had various barriers that could potentially be lessened with the support of family members, especially their wives, peers, and healthcare providers (Tungtrongvisolkit & Seaharattanapatum, 2021). However, existing knowledge within the Thai context lacks a comprehensive understanding of pregnant women’s perspectives. The specific views of pregnant women on passive smoking, as well as their capabilities, challenges, and needs in managing their husbands’ smoking, remain unclear. To address this gap, a qualitative study was undertaken to explore prenatal passive smoking at home based on the experiences of women in Thailand. The resulting insights contribute new knowledge for nurses and healthcare professionals that can be applied in the development of practice guidelines, aligning with the women-centered approach that has been recommended for a decade (World Health Organization, 2013).
Methods
Study Design
This study employed a qualitative descriptive approach as it provides a comprehensive summarization, in everyday terms, of specific events experienced by individuals (Lambert & Lambert, 2012). Data collection was guided by naturalistic inquiry to elicit and capture testimonies of individuals’ unique experiences about practices (Sandelowski, 2000). The individual is a being in which things have value and significance; thus, they cannot be eliminated but taken into constituting their reality. This study focused on non-interpretive inquiry, presenting the findings in everyday language rather than conceptual, philosophical, and abstractive words (Sandelowski, 2000).
Participants
The participants were purposively recruited from postpartum units, family planning clinics, and well-baby clinics of five hospitals to obtain the diversity of socioeconomic status. Initially, nurses screened the potential participants who reached the inclusion criteria through their health records. The criteria included the mothers who had experienced prenatal passive smoking at home, aged 18-35 years, and had already given birth for two months or less. If the women expressed their interest, the nurses asked for permission to contact them by the first author via telephone. After the telephone conversation, a face-to-face contact was arranged to explain the research details and reasons for doing the research. Data saturation was reached at 16 participants, where no new information was obtained from the interviews (Lincoln & Guba, 1985).
Data Collection
Data were collected between September 2020 and April 2022 in Chiang Mai City, northern Thailand. This study was reported following the Consolidated Criteria for Reporting Qualitative Research (COREQ) (Tong et al., 2007). Prior to the study, no relationships existed between the researcher and participants. Rapport was built throughout the study until the interview closure. The interviews were carried out by the first author, a female PhD candidate and a nursing instructor experienced in supervising antenatal clinics. Semi-structured in-depth interviews were carried out in Thai for 2-3 sessions lasting 40-80 minutes for each interview in the hospitals’ counseling rooms or the participants’ houses where no one other than the participants and the first author were present. The interviews followed the semi-structured interview guide using broad issues and open-ended questions: “Please tell me about your husband’s smoking at home while you were pregnant,” and “What did you do during your pregnancy about your husband’s smoking at home?” Next, probing techniques were employed. A reflective journal was written before and immediately after the interviews. The interviews were audio-recorded and transcribed verbatim in the Thai language.
Data Analysis
The data were analyzed manually using seven steps of thematic analysis (Sandelowski, 2000) by the first author under the supervision of dissertation committees. The steps included 1) listening to the participants’ voices repeatedly; 2) transcribing the interviews verbatim; 3) reading and re-reading the transcriptions several times to understand the entire transcriptions; 4) describing data into codes; 5) classifying codes into sub-themes; 6) identifying similar sub-themes within the themes; and 7) reviewing and refining sub-themes and themes by comparing all types of data. In the final step of data analysis, the findings were translated into English.
Trustworthiness
The trustworthiness of this study was achieved through credibility, transferability, dependability, and confirmability (Lincoln & Guba, 1985). In credibility, peer debriefing and member checking were conducted. Peer debriefing involved meeting with two experts twice: one to examine the research processes and methods and the other to discuss the tentative findings. Member checking can involve presenting data transcripts or data interpretations to all or some participants (Holloway & Galvin, 2017; Varpio et al., 2017). In this study, tentative themes were presented to three participants and discussed; contradiction was not found. In confirmability, reflective journals for self-awareness were written before and immediately after the interviews to examine and remind the researcher’s feelings, thoughts, and potential bias and to guide the next interview session. Auditing all research processes and documents also ensured dependability and confirmability. Data analysis, findings, and interpretations were discussed with the advisory committee. Transferability was also achieved through the thick description of the findings.
Ethical Considerations
This research was approved by the Research Ethics Committee of the Faculty of Nursing, Chiang Mai University (Study Code: 2020-EXP065) and by the target hospitals. The participants obtained information about the research project, its risks and benefits, and their rights, and gave written consents. All personal details were held confidential and respected. The principles of the Helsinki Declaration were maintained. The participants received compensation of 100 baht (2.86 USD) per each interview for their time. Due to the COVID-19 situation, the authors performed the prevention measures of COVID-19 transmission.
Results
All 16 participants remained in the study. They were married, aged 20-35 years. Ten participants finished senior high school or lower. Their family income varied from 6,000 to 40,000 baht/month (171.53 -1,143.51 USD). Two participants worked in relation to health: a traditional Thai medical professional and a health volunteer. Nine participants lived in rural areas. Ten participants lived in an extended family. Seven participants had one living child, while nine had 2-3 living children. Three participants had their newborns with some complications, such as low birth weight, preterm delivery, jaundice, or asthma. Seven participants received antenatal education on prenatal passive smoking. Twelve participants reported their husband as the only smoker in their family. During the prenatal period, 11 husbands had never stopped smoking; 3 husbands were successful in ceasing smoking. None of the husbands attended a smoking cessation clinic.
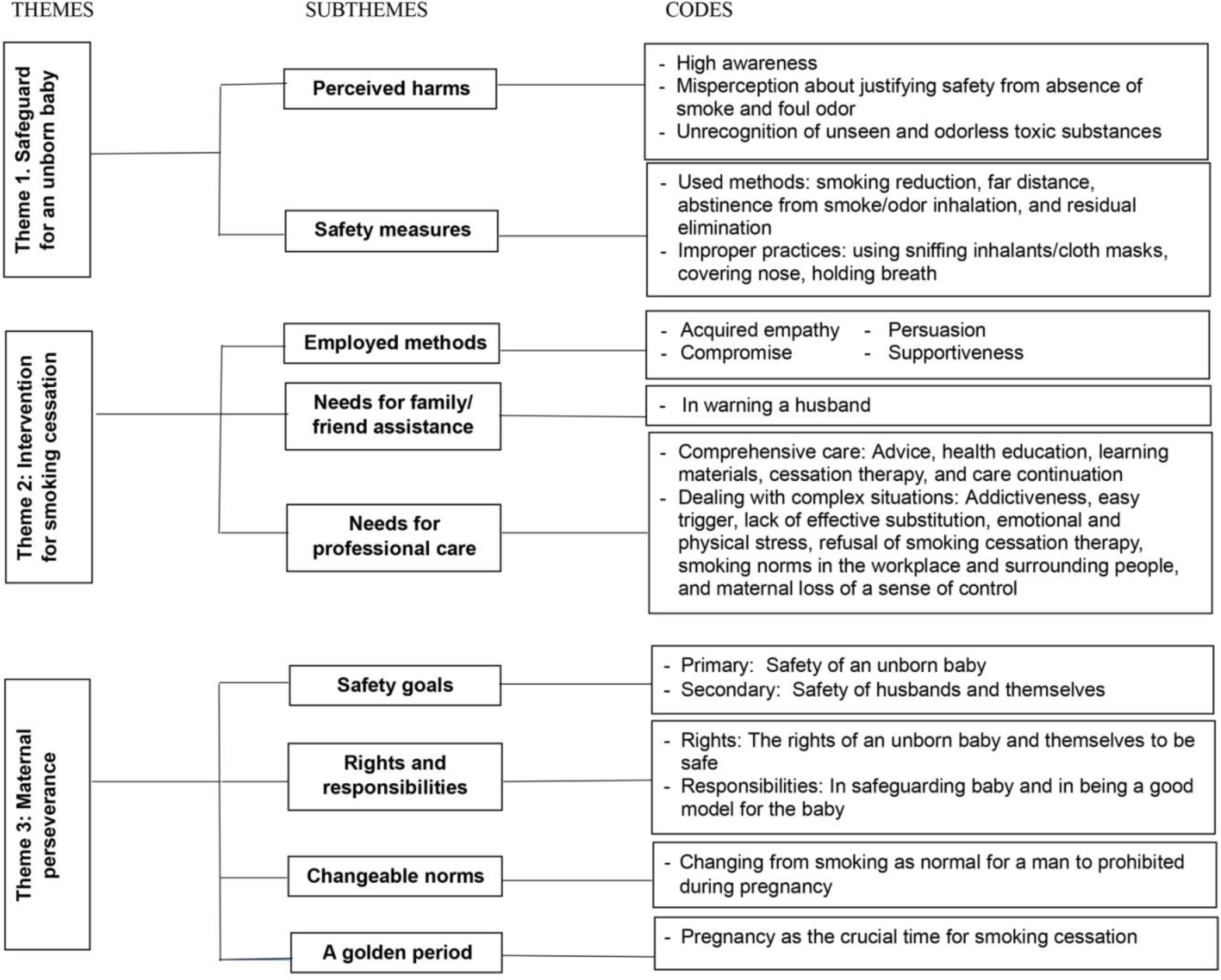
All participants were highly aware of passive smoking, but most of them misperceived safety from the absence of smoke and foul odor, unrecognizing unseen and odorless substances. They safeguarded their unborn babies through various safety measures, which some practices were improper due to their misperception. To achieve the final goal of ending the husband’s smoking, several interventions were employed, but they still needed assistance from their family/friends and healthcare providers. Throughout their challenging journey to pursue safety and smoking cessation, their perseverance was crucial. Three themes and nine subthemes emerged, as illustrated in Figure 1. The presented findings were confirmed anonymously by the participants’ quotes and identification numbers. P1 means the quote from the participant whose identification number was 1.
Theme 1: Safeguard for an unborn baby
The participants protected their unborn babies from harm inflicted by smoking based on their perception of the damages of passive smoking, using various measures to prevent the baby from smoking exposure.
Subtheme 1.1: Perceived harms
Home passive smoking was perceived to cause several harms to the unborn baby, such as lung damage or diseases, asthma, allergy, poor brain development, learning disability, low intelligence, small babies, and even death. Compared with THS, SHS was better known and believed to be more harmful. SHS was less dangerous than first-hand smoking (FHS), but one participant (P1) had a contradiction, as she rationalized, “The smoker got little disadvantages because he sniffed and then blew out. We’re being there. We sniffed, but we didn’t blow out.”
Unfortunately, the things causing harm were misperceived to be smoke and the foul odor of cigarette smoke entering the body by breathing, which the smoke was more harmful than the foul odor. Interestingly, many of them did not recognize some toxic substances. The smoke and odor could remain in bodies, walls, curtains, chairs, and inside houses and cars. How to jeopardize the baby was unclearly explained. For example, one (P16) said: “I don’t know about the substances in tobacco, but I know that cigarette smoke and foul odor are harmful.”
Subtheme 1.2: Safety measures
High awareness of harm led to the participants’ attempt to safeguard their unborn babies through smoking reduction in number and frequency. Keeping a far distance, including smoking at the workplace, outside, and in the downwind direction, and walking away were attempted as far as they did not sense any odor or smoke. Abstinence from smoke/odor inhaling was practiced through the following: covering the nose, closing windows or doors, holding the breath, putting on a face mask, or turning on air purifiers. Unfortunately, sniffing inhalants and using cloth masks were mentioned, for example: “I would sniff the inhalants to reduce the smoke smell.” (P4); “I used a cloth mask because I smelled smoke less than a hygienic one. A cloth mask was thicker, so it prevented cigarette smoke more than a hygienic mask did” (P8).
Additionally, residual elimination was practiced through taking a bath and a shampoo, handwashing, changing clothes, leaving clothes outside the room, washing clothes separately, brushing teeth, rinsing mouth, drinking water, and eating candy. However, washing curtains, cleaning furniture, or cleaning inside cars were not mentioned.
Theme 2: Intervention for smoking cessation
The participants used four methods in intervening with their husband’s smoking. However, they still needed assistance from their family/friends and healthcare providers.
Subtheme 2.1: Employed methods
Four methods, including acquired empathy, persuasion, compromise, and supportiveness, were used to stop their husbands’ smoking. Firstly, devastating emotions of sadness, disappointment, and anger, as well as hardship, were expressed to acquire the husband’s empathy, wishing him to quit smoking. For example, one (P12) said: “I told him I’m sad. He said he understood, but he still smokes as usual.” Secondly, persuasion was employed by having the husband think logically about stopping doing harm, doing good things, and being a good model for the baby. “If you smoke, it hurts the baby. You’re already a dad. You have to stop for the baby.” (P6); “Smoking is a bad model for the kid. I told him if he could quit, then quit.” (P3). Thirdly, when quitting immediately was unlikely to be successful and may bring hardship to their husbands, they frequently compromised by being satisfied with just reducing the smoking gradually. Instead of using pressure and coercion, they tried to understand and encourage their husband. For example, one (P4) said, “From smoking to no smoking, it makes him irritable. I tried to be less emotional with him but encouraged him.” The critical reason for compromising was to maintain their marital stability, as one (P2) said, “I tried to speak nicely. I don’t want to have a family matter.” Finally, being mentally supportive was expressed in several ways to help the husband keep his pursuit as one (P9) said, “I often admired my husband after he could reduce smoking. Always admired him.” Another participant (P10) also advised, “I spoke to comfort him. It doesn’t matter. Take a candy.”
Subtheme 2.2: Needs for family/friend assistance
Needs for family/friend assistance was rationalized as “I want someone’s help to tell my husband to quit or lessen smoking. It seems like many voices can help. Only my voice is low.” (P13). Their family and friends helped them by warning their husbands to stop smoking. The initiation of warning could help them further dare to deal with the husband as one (P7) said, “His relatives told him to quit smoking. When I heard that, it gave me the courage to speak up and add on it.” However, home smoking by the participant’s father (P2), close relationships between the husband and his mother or grandmother (P3, P6), and friends’ smoking were the barriers in warning. In contrast, senior family members could help in making a deal with the husband to quit smoking (P6). The participants were also supported by being reminded to stay far away from cigarette smoke (P4).
Subtheme 2.3: Needs for professional care
The following statements revealed the participants’ dissatisfaction with healthcare services, leading to their need for adequate and comprehensive care: “In health education, it talked roughly about dangers of smoking in general.” (P6); “They just roughly told me to have my husband stop. But they didn’t tell the ways.” (P3). Their needs included more advice in person and health education classes, more smoking cessation therapy, continuation of care, and written learning materials. They suggested a booklet or QR code (P16); internet applications containing pictures and texts (P4); VDO clips and pictures (P3); a group of moms on Facebook or a line group managed by healthcare providers (P7); and skillful educators (P16). “I wanted some materials explaining the impacts and giving knowledge by healthcare providers. It should be concrete rather than abstractive materials. VDO rather than lecturing. There should be things to explain about lungs. It helps us to see clearly” (P1).
They also needed assistance in dealing with various complex situations beyond their capability, including addictiveness, easy triggers, lack of effective substitution (such as keeping busy, eating candy, and eating desserts), emotional and physical stress, refusal of smoking cessation therapy, smoking norms in the workplace and surrounding people, and maternal loss of a sense of control. These are some examples of their expression: “I really want to take my husband to smoking cessation clinic. I asked him to go, but he wouldn’t go. I asked him to go, but he said it’s complicated.” (P10); “I can control many things. But the only thing I can’t control is that he smokes secretly” (P6).
Theme 3: Maternal perseverance
The participants’ narratives about their substantial efforts and endurance for a long period despite the hardship in their attempts to terminate their husband’s smoking were interpreted as their perseverance. “I kept telling him continuously. I never felt discouraged because the ones who can quit smoking take much time. Some try so hard; need time. Some cannot quit. I think it isn’t easy. If we keep telling him every day, he’ll come to terms with us” (P3).
Their perseverance was influenced by four motives described in the following subthemes.
Subthemes 3.1: Safety goals
The safety of an unborn baby was a primary goal developed from maternal instinct. The safety of husbands and the participants themselves was the secondary goal. “I’m indeed a mom. I want to protect my baby. I must tell my husband that it’s time to quit smoking” (P10); “I told him to reduce smoking gradually for our baby’s health and his health as well” (P15).
Subtheme 3.2: Rights/Responsibilities
One participant (P10) stopped intervening with her husband and reasoned that it was her husband’s right to smoke, “If he wants to smoke, he can. I think it’s his personal matter. It’s his right.” Another participant (P13) wanted providers’ explanation about the rights of smoking, “I want advice if I meet smokers. What should I do to be safe? Like the rights of the smokers and the rights of the ones who don’t smoke.” The belief in fetal and maternal rights to be safe acquired the participants’ attempt and insistence to stop their husband’s smoking. In addition, it was believed that a father had to be responsible for and dedicated to his baby’s well-being and safety by ceasing smoking, as one (P6) said, “You’re already a dad. You must do everything good for the baby.” She felt that she took responsibility as a mother, but her husband was irresponsible as he continued smoking.
“When I was pregnant, I took care of myself. I was careful about food, eating, and anything for my health because I had difficulty getting pregnant. He promised to do it for the baby’s sake, but he couldn’t” (P6).
Subtheme 3.3: Changeable norms
Before having a baby, some participants accepted the norm of male smoking. “Smoking’s normal in general. My neighbor also smokes. I thought it was normal as well. I don’t mind his business. He smokes as wants.” (P4). However, they changed their point of view on smoking norms when they got pregnant. Smoking became prohibited, leading them to stop their husband’s smoking. “When I wasn’t pregnant, I felt indifferent about smoking. I had no sense of being a mother. Once I got pregnant, I feel cigarette smoke is so harmful to the kid” (P4).
Subtheme 3.4: A golden period
Before having a baby, some participants had never told their husbands about smoking cessation, but they did when they were pregnant, as they said: “At that time, I might not have thought because I was alone, I wasn’t pregnant.” (P16); “When I knew I was pregnant, then I talked about lowering the smoking.” (P9). The participants and their husbands considered pregnancy as an excellent time for ceasing smoking: “It is time to quit smoking.” (P10); “I thought it’s a baby. Having a baby, he lessens his smoking. It makes him realize about having a little baby” (P3).
Their anticipation of having a baby and being expectant parents induced them to contemplate smoking cessation. The main reason was to safeguard their unborn baby. Another reason was to be a good model for the baby. Not only the prenatal period, but some participants also dealt with their husbands before (P1) or after (P9) they were married. One participant (P4) set the stipulation with her husband that they would plan to have a baby only if his smoking stopped. Most of them used the pregnancy period as the time to stop their husband’s smoking. However, two participants (P7, P14) expressed that their husbands had negotiated to quit after their baby was born. One reason might be that the baby was still unseen inside the womb. “When he saw the kid as the person, he might feel the need to quit. But when the baby was inside the belly, it wasn’t clearly seen as a person, sort of” (P7).
Discussion
Prenatal passive smoking at home based on the experiences of women emerged into three themes. The first theme focused on safeguard for an unborn baby. The harm of SHS was perceived to result from smoke and odors, which resonated with another qualitative study among Thai pregnant women (Tantanokit et al., 2023). The participants were unlikely to recognize specific toxic chemicals and how they jeopardized the baby. Approximately, 85% of the 4,000 toxic chemicals in tobacco are invisible and odorless and can pass through to an unborn baby (The National Health Service, 2023). Carbon monoxide, tar, cadmium, nicotine, and other compounds cause fetal hypoxia, reduced uteroplacental blood flow, and direct toxic effects, resulting in adverse outcomes (Cunningham et al., 2022; McDonnell & Regan, 2019). The child’s health problems included sudden infant death syndromes, respiratory infections, ear infections, and asthma (Centers for Disease Control and Prevention, 2022b).
SHS was perceived to be less harmful than FHS. SHS has the same toxic chemicals that people who smoke inhale (Department of Health and Aged Care Australia, 2019). The causes of harm from THS were also cited as smoke and odor sticking on clothes and paternal bodies. The particles in SHS can remain in dust and on surfaces for months after the smoke disappears, which can be swirled up and inhaled or orally taken (American Cancer Society, 2023). The unrecognition of toxic chemicals in tobacco and inaccurate understanding of the effects of each type of passive smoking were probably because less than half of the participants received antenatal education on passive smoking. Thus, these issues should be incorporated into antenatal health education. Nurse-midwives should emphasize the potential misunderstanding of harm of passive smoking from unseen and odorless chemical substances, especially from THS.
The participants performed several safety measures to safeguard their unborn baby from prenatal passive smoking. However, some practices were improper since unseen and odorless harmful substances were poorly understood. The recommendations to improve indoor air quality are source control, improved ventilation, and air cleaners (The United States Environmental Protection Agency, 2023). In controlling smoke, all of them had their husband smoke outside, which was hard to determine how far and how long, and then falsely determined safety by counting on the absence of smoke and odor. There is no safe level of exposure to SHS; smoking outside and indoors has the same adverse health effects; the only difference is that the concentration of chemicals is higher, and it remains longer indoors (The United States Environmental Protection Agency, 2023). These messages should be sent to pregnant women. In addition, sniffing inhalants used in our study might hide the smell of smoke, but they cannot eliminate harmful toxins (The National Health Service, 2023). Cleaning curtains and furniture can eliminate some residual substances, but no participants mentioned them.
The second theme involved the intervention for smoking cessation. Correspondent with some previous studies, the participants employed various methods by expressing devastating emotions of sadness, disappointment, and anger, as well as hardship, to acquire the husband’s empathy, wishing him to quit smoking. Considering the methods employed for ending smoking, activating empathy (Shen, 2015), explaining the health problems of unborn babies and children (Ayuningtyas et al., 2021a; Tungtrongvisolkit & Seaharattanapatum, 2021), and being supportive (Ayuningtyas et al., 2021a) were also reported. Persuading their husbands by drawing upon doing good things or being a good model for the baby was supported by the finding that ex-smoker husbands who quit smoking rationalized that they did not want their children to smoke like them (Ayuningtyas et al., 2021b). Interestingly, our study findings were supported by the previous studies in Thailand in terms of the fear of jeopardizing their marital relationship (Ayuningtyas et al., 2021a) and relying on their husband’s conscience to quit when no changes in their husband’s smoking behavior (Ayuningtyas et al., 2021b). This suggests that, in the Thai context, nurse-midwives should advocate pregnant women’s intervening methods with husband’s smoking while keeping in mind the importance of maintaining marriage stability.
The participants mentioned their need for assistance from their family/friends and providers. Consistent with the literature, children (Ayuningtyas et al., 2021a), friends (Seo et al., 2021), and family (Soulakova et al., 2018) were helpful in stopping the husband’s smoking. However, the participants did not put much effort into requesting their help, possibly due to the perception that marital issues were a private matter in which no one should get involved. Nurse-midwives should empower pregnant women to assertively tell their family, friends, and co-workers to support their husbands in smoke cessation for their own baby’s sake. Nurse-midwives can encourage their family and friends to contribute to warning their husbands to quit smoking by distributing written information to these potential assistants.
In addition, similar to our findings, women described the limitation in information, written materials, strategies, and approaches to SHS exposure, leading to the need for expert counsel, subject-specific education, and training (Artzi-Medvedik et al., 2022). Pregnant women needed their providers to maintain and enhance their perseverance in pursuit, particularly in encouraging their husband’s attendance to smoking cessation therapy, which also echoed previous research (Faseru et al., 2018). This indicates that nurse-midwives should provide comprehensive details on passive smoking using various media to provide concrete knowledge in a clear picture. Health education provided through brochures, videos, and electronic media could effectively enhance pregnant women’s access to information and increase their knowledge of SHS (Abu-Baker et al., 2022). Nurse-midwives can also offer counseling on how to deal with complex situations in intervening with the husband’s smoking, which can lead to the husband’s tobacco reduction (Wahabi et al., 2020).
It is known that intervening with the husband to quit smoking is the woman’s hardship. Interestingly, our study found that maternal perseverance, reflecting their prolonged endurance despite the hardship in their effort, was the critical element in continually pursuing their husband’s smoking cessation. Importantly, their ways to acquire, maintain, and enhance their maternal perseverance can be applied by nurse-midwives in assisting women when they feel discouraged and desperate. Pregnant women in Malaysia tried to stop their husbands smoking due to their maternal instinct to protect their baby’s health and their concerns about their husband’s health (Asri et al., 2017). Similarly, our study found that the safety of an unborn baby was a primary goal influenced by maternal instinct, followed by the safety of their husband and the participants themselves.
Rights and responsibilities were another motive to attempt to stop smoking at home. Being unharmed is a basic human right. Pregnant women should understand and assert their right to a smoke-free environment at home and protect their baby’s right to be safe at home. In Thailand, according to the Promotion of Development and Protection of Family Institution Act, B.E. 2562 (2019), smoking in the home is considered an act of domestic violence with the intention to harm health (The Royal Thai Government Gazette, 2019). Therefore, pregnant women’s knowledge and understanding of relevant laws will enhance their rights awareness. Considering paternal responsibility, a father had to be responsible for and dedicated to their baby’s well-being and safety by ceasing smoking.
Similarly, fatherhood-related perceptions and responsibilities could shape fathers’ views of their role in creating and maintaining a smoke-free home (ODonnell et al., 2019). Thus, smoking fathers should be included in health education and nursing interventions to raise their awareness of their responsibility to be involved in the care and protection of the unborn baby by reducing or quitting smoking. Consistently, family counseling that included both pregnant women and their smoking husbands provided an opportunity for nurses to train future fathers to ensure smoke-free environments for their families (Soltani et al., 2019).
Changeable norms were reflected when the participants initially internalized the norm of smoking as normal for men, but they changed their point of view on smoking once they became pregnant. Consistently, Chinese wives held negative attitudes toward their husbands’ smoking and often asked their husbands to quit (Mao et al., 2015). Another motive was a golden period, as pregnancy was an optimal time for ceasing smoking. This resonates with the notion by the World Health Organization (2013) that pregnancy is theorized as a “teachable moment” for women when their perception of health risks is considerable. Pregnancy is a time of preparedness and tobacco cessation, not only for women but also for their partners and other people living in their households. Consistently, the birth of a child and planning to conceive were found to be highly influential on the wives’ enforcement of rules to restrict their husband’s smoking (Ayuningtyas et al., 2021a). Thus, nurse-midwives should educate and provide valuable resources for pregnant women as empowerment to enhance self-advocacy, confidence, and perseverance to continue until their husbands succeed in quitting smoking.
This study had some limitations. Most participants had a low socioeconomic status and might internalize traditional beliefs about conforming to their husbands and family. It might be hard to address the husband smoking at home. They might be limited in accessing passive smoking information. Women from other backgrounds may hold different viewpoints and have different experiences. Further research may explore pregnant women’s views in other contexts to broaden the insights into this phenomenon.
Conclusion
The findings provided three themes from the experiences of women on prenatal passive smoking at home, including safeguard for an unborn baby, intervention for smoking cessation, and maternal perseverance. This new knowledge is beneficial in developing practice guidelines for caring for pregnant women who experience passive smoking at home based on a women-centered approach. Comprehensive professional care should be refined, including advice, self-learning materials, health education, smoking cessation therapy, continuation of care, and assistance for dealing with complex situations. Unseen and odorless substances found in passive smoking that jeopardize an unborn baby and the effective methods for exposure prevention should be highlighted. Nurses and midwives should encourage women’s perseverance to continue until their husbands succeed in quitting smoking.