










Background
In some areas of Liberia and sub-Saharan Africa, the Ebola virus disease (EVD) outbreak has resulted in widespread suffering and fatalities (Ali et al., 2020). Depending on the species, EVD has historically had the highest case fatality rate, ranging from 50% to 90% (MacNeil & Rollin, 2012). Since 2000, the number of EVD outbreaks and cases on the continent has significantly increased (Kobayashi et al., 2015). This can be partially attributed to the continent’s fast population growth and increased human contact with wildlife with host species like monkeys, bats, and chimpanzees in formerly pristine forest environments (Brainard et al., 2016). Bats are believed to carry a classic zoonosis EVD; however, this is not confirmed (Selvaraj et al., 2018).
EVD, especially among healthcare workers (HCWs), has been a significant driver of its transmission since the first human outbreaks were reported in 1976 (Abramowitz et al., 2018). Without proper precautions, bodily fluids from a sick or deceased person can spread the Ebola virus, making infections common (International Ebola Response Team et al., 2016). HCWs are more likely than the general public to become infected with EVD during an outbreak due to their frequent close contact with patients and possible exposure to infectious fluids (Furuse et al., 2017). During the West African outbreak of 2014–2016, at least 3 percent of EVD cases among HCWs occurred, and 66 percent of those cases were fatal (Koepsell et al., 2023). Furthermore, young adults are especially susceptible to the far-reaching effects of EVD, especially in its early stages when the virus is most easily transmitted (Wiratsudakul et al., 2016). Challenges with clinical recognition and the requirement for diagnostic capabilities are obstacles to implementing universal precautions to prevent exposure in settings with limited resources. Inadequate training, inadequate public health infrastructure, and inadequate personal protective equipment, such as gloves, gowns, and face shields, are further challenges (Dokubo et al., 2018).
Even though a disproportionate number of EVD cases during previous outbreaks have been from the Liberian population, not all of them get sick despite having a lot of contact with infected patients. Estimates of the prevalence of EVD in people with no or few symptoms range from 1.0 percent to 45.8 percent, depending on the population, sampling strategy, time, place, and assay (Mbala-Kingebeni et al., 2021). If even subclinical infection results in immunity, a high infection rate that produces no symptoms could significantly impact population health (Bisimwa et al., 2022).
Death related to traditional burial in EVD has been seen only in remote parts of Liberia’s central and southeastern rural areas since 2014. On the other hand, between 2014 and 2016, EVD spread from West African rural to urban areas (Carter et al., 2018), killing over 11,000 people in Guinea, Sierra Leone, and Liberia (Casey et al., 2015). When the epidemic struck all three countries in 2014, people had limited access to healthcare due to a lack of infrastructure, resources, and experience managing EVD. Weak health systems and high levels of community mobility are just two elements connected to the sharp rise in the scope of the West African epidemic (Reichler et al., 2018). As noted by Brown et al. (2018), explanations that more accurately reflect the real world will require these kinds of justifications in addition to an alternative set of criteria, specifically those directly based on the historical trajectory of the area.
The role of nurses in anticipating the potential risks components and conducting prevention measures for the Ebola virus outbreak in Liberia is critical. Nurses are on the front lines of patient care, and their perspectives are invaluable in understanding the challenges that arise during outbreaks, implementing effective prevention measures, and providing the best possible care to those affected (Matlock et al., 2015).
This study’s in-depth interviews with health workers, including nurses and stakeholders, allow for a comprehensive exploration of their experiences, perceptions, and expertise. With their frontline experience, nurses can offer unique perspectives on the challenges faced in dealing with Ebola, the risks encountered, and the effectiveness of various prevention measures (Paillard-Borg et al., 2020).
The Ebola outbreak highlighted significant global healthcare disparities and the urgent need for Liberia’s healthcare system to be improved. Several international aid organizations worked to identify Ebola cases, treat them, and prevent further transmission. However, little research has been conducted on the perspectives of healthcare workers, including nurses and stakeholders, on EVD since the epidemic ended in early 2016. Our study seeks this gap by exploring the real-life experiences of stakeholders and healthcare professionals in Liberia. It is dedicated to understanding these individuals’ views, attitudes, and beliefs concerning Ebola. Interviews were conducted with stakeholders and healthcare workers who observed the epidemic. This study aimed to explore the potential risk components and prevention measures from stakeholders and healthcare workers to help inform future intervention strategies for EVD in Liberia.
Methods
Study Design
The study used an exploratory, descriptive qualitative design that prioritized understanding, meaning, and actual human experiences (Hunter et al., 2019). This design is essential for comprehending a real-life scenario in its natural context (Sandelowski, 2000). This study also adhered to the 32-item Consolidated Criteria for Reporting Qualitative Research (Tong et al., 2007). Furthermore, the dense data descriptions in the study allowed for a better understanding of healthcare workers’ and stakeholders’ perspectives on the potential risk components and prevention measures of EVD.
Participants
Twenty of thirty participants, consisting of nurses and medical doctors, were purposefully recruited based on their level of experience with the EVD. Inclusion criteria included: 1) health stakeholders in Liberia who had laboratory-confirmed Ebola virus infection and been cured, and 2) frontline health workers in Liberia who had laboratory-confirmed Ebola virus infection and been cured. Exclusion criteria included: 1) who refused to grant permission for an interview and 2) who was above 65 years old and had not experienced the outbreak. We recruited stakeholders and health workers due to their expertise in public health management or nursing practices.
Data Collection
Data were collected from February 2022 until August 2023. The primary data was gathered through open-ended (in-depth) interviews with participants scheduled to last 60-90 minutes. An interview guide guaranteed methodological consistency throughout the data collection process. Each participant was interviewed by two researchers (MTS and PCD). The semi-structured face-to-face interview reflected the risk components and preventative measures associated with the EVD outbreak. At the start of the interview, basic demographic information was gathered. We initially estimated a sample size of approximately 30 participants, but after determining eligibility criteria, 20 participants were selected to achieve data saturation. The study interviews were conducted at the Redemption hospital, J.F.K hospital, and the Ministry of Health in Liberia. All interviews were conducted in English since the participants were fluent in English.
Participants were asked to describe their experiences during and after the Ebola virus outbreak, potential risk components, and prevention measures. Depending on the interview, further follow-up questions were used for clarification when needed, such as “Can you tell me more about that?”, “Can you give an example of what you have just said?”, “What is your opinion on that?”, “What concerns do you have about that?”, “What kind of support did you receive?”, “What is your evaluation of what has been done?”, and “What do you propose/expect?”.
During face-to-face interviews, a Sony digital flash memory voice recorder and phone recorder were employed to document each conversation. We systematically recorded and stored all spoken interactions using a computer as an integral step in the data collection. Consequently, verbatim transcriptions of the data were generated following each interview.
Data Analysis
NVivo 12 Plus was used to import the transcript results and finish the iterative analysis process (Aspers & Corte, 2019). Thematic development was made possible by the creation of nodes (codes) from gathered data. The following steps were involved in the inductive thematic analysis of the data: becoming acquainted with the data, creating preliminary codes, looking for themes, evaluating themes, defining and labeling themes, and completing the report (Bingham & Witkowsky, 2021; Nowell et al., 2017).
Following the data segmentation into Nodes (codes) and cases, NVivo 12 plus software was used to establish themes. Subsequently, the data analysis involved reading individual paragraphs, sentences, and lines of text to comprehend the implications of the EVD outbreak on potential risk components and prevention measures in Liberia. Consequently, we achieved data saturation after addressing each theme or node (Fusch & Ness, 2015). Data saturation, therefore, required that each preset theme be modified repeatedly (Aspers & Corte, 2019). The authors actively participated in in-person discussions during the data analysis to confirm major themes and subthemes.
Trustworthiness/Rigor
In qualitative research, trustworthiness is defined by Korstjens and Moser (2018) as authenticity, confidence, and credibility. We used an electronic audio recorder to record each semi-structured interview to ensure the study’s validity. The interview was repeated to determine the study’s rigor. Each participant’s interview was evaluated for credibility, dependability, and transferability. In addition, an audit trial was carried out to ensure credibility during data collection. To ensure that the interpretation was founded on the participants’ reports, the transcript was returned to all 20 participants for any revisions or comments they wished to add before data coding. Every participant concurred with the key issues that were outlined. We assessed the findings’ transferability by using appropriate participant selection, data collection, analysis, and relevant quotations.
Ethical Considerations
The Faculty of Medicine at Universitas Airlangga provided an ethical approval certificate (29/EC/KEPK/FKUA/2023). Before handling the research tool, participants signed a consent form outlining their rights, obligations, and the purpose of the study. Participants’ privacy would be protected, and their information would never be sold to a third party for profit. Participants were also informed of their right to withdraw from the study and that their participation was voluntary.
Results
Participants’ Characteristics and Interview Duration
The findings of the qualitative study were based on interviews with twenty participants from various sectors, including hospitals and the Ministry of Health. The participants were healthcare workers and health stakeholders; they were experts and provided vital information that was reliable and very important to be considered in better management of EVD (Table 1). The age of participants ranged from 30 to 65 years old. They hailed from across Liberia, with 12–34 years of government health service and clinical professional experience (Table 2).
| Participants | Sex | Workplace | Profession | Duration of interview |
|---|---|---|---|---|
| Participant 1 | Male | Ministry of Health | Dermatologist | 1 hour 30 min |
| Participant 2 | Male | Ministry of Health | Microbiologist | 1 hour 30 min |
| Participant 3 | Male | Ministry of Health | Pathologist | 1 hour 30 min |
| Participant 4 | Male | Ministry of Health | Dermatologist | 1 hour 30 min |
| Participant 5 | Male | Redemption Hospital | Microbiologist | 1 hour 30 min |
| Participant 6 | Male | Ministry of Health | Psychiatrist | 1 hour 30 min |
| Participant 7 | Male | Redemption Hospital | Microbiologist | 1 hour 30 min |
| Participant 8 | Male | Redemption Hospital | Anesthesiologist | 1 hour 30 min |
| Participant 9 | Male | J.F.K Hospital | Oncologist | 1 hour |
| Participant 10 | Male | J.F.K. Hospital | Immunologist | 1 hour 30 min |
| Participant 11 | Male | Redemption Hospital | Dermatologist | 1 hour 30 min |
| Participant 12 | Male | Redemption Hospital | Pathologist | 1 hour |
| Participant 13 | Male | Redemption Hospital | Immunologist | 1 hour 30 min |
| Participant 14 | Male | J.F.K. Hospital | Microbiologist | 1 hour 30 min |
| Participant 15 | Male | Redemption Hospital | Microbiologist | 1 hour 30 min |
| Participant 16 | Female | Redemption Hospital | Pediatric Nurse | 1 hour 30 min |
| Participant 17 | Female | Redemption Hospital | Pediatric Nurse | 1 hour 30 min |
| Participant 18 | Female | Redemption Hospital | Psychiatric Nurse | 1 hour 30 min |
| Participant 19 | Female | Redemption Hospital | Maternal and child Nurse | 1 hour 30 min |
| Participant 20 | Female | Redemption Hospital | Maternal and child Nurse | 1 hour 30 min |
| Participant Groups | Number (n) | Sex | Age group (years) | City | |||
|---|---|---|---|---|---|---|---|
| Male | Female | 30-46 | 47-56 | 57-65 | |||
| Health Stakeholders | 5 | 5 | 0 | 1 | 2 | 2 | Monrovia |
| HCWs | |||||||
| Doctors | 10 | 10 | 0 | 3 | 4 | 3 | |
| Nurses | 5 | 0 | 5 | 2 | 2 | 1 | |
| Total | 20 | 15 | 5 | 6 | 8 | 6 | |
Thematic Findings
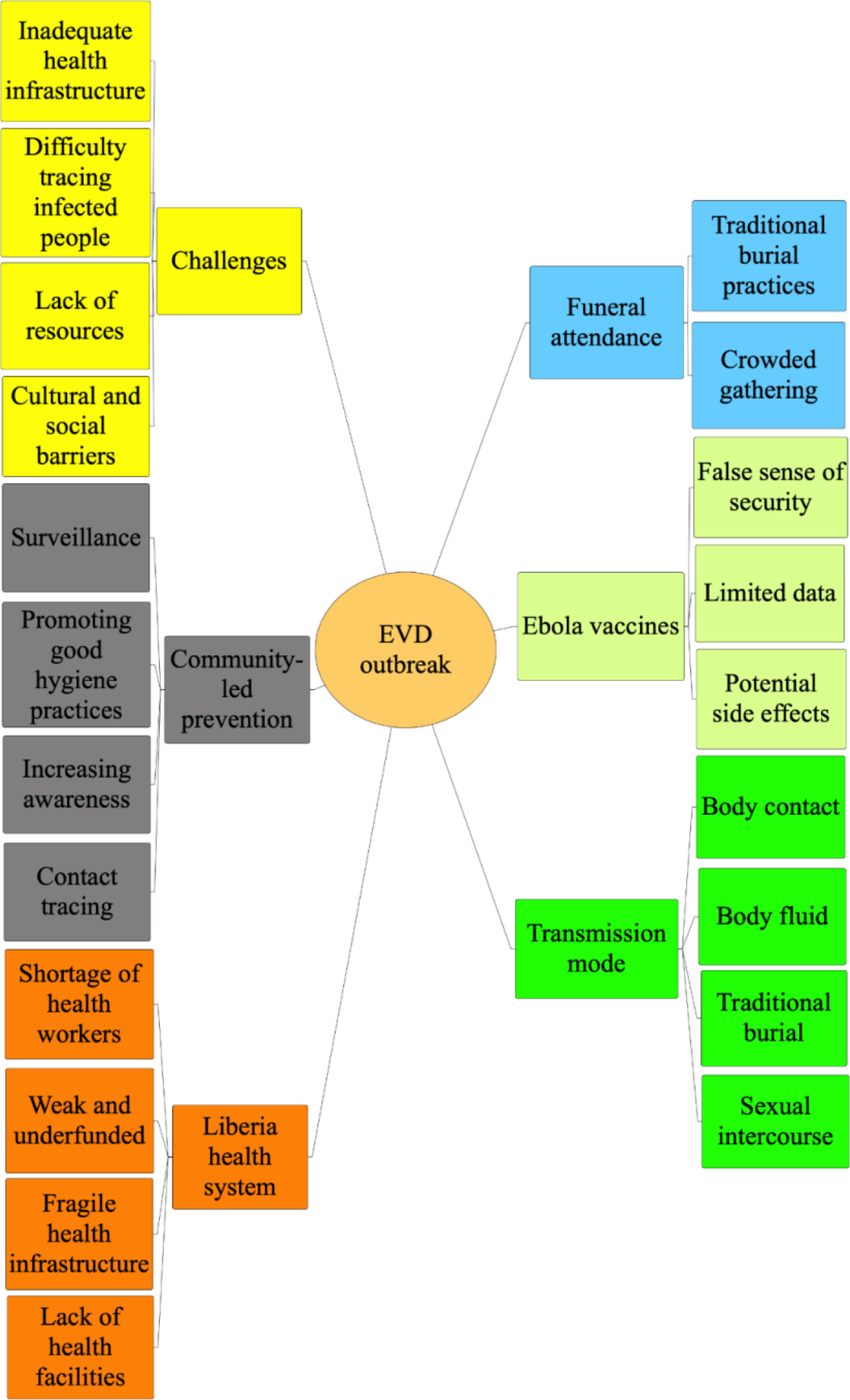
Six major themes emerged, known as the parent nodes, and 21 subthemes are referred to as child nodes (Figure 1). The mind map shows the relationships between different pieces of the obtained data to make the structure of the nodes from the six emerging themes: transmission mode, funeral attendance, community-led prevention, Ebola vaccine, challenges in implementing prevention measures, and Liberia’s health systems. Some participants expressed the same thought in each theme, so only one representative quote and any participants who provided a similar thought are shown.
Theme 1: The transmission mode of EVD outbreak
This theme is comprised of subthemes like body contact, body fluid, and traditional burial, sexual intercourse. The transmission mode of the Ebola virus had to be critically monitored, including direct contact with the bodily fluids of an infected person showing symptoms of the disease, such as blood, vomit, urine, feces, saliva, and semen.
The participants’ quotes can be seen in the following:
“Yes, it is primarily transmitted by direct touch with an infected person’s bodily fluids. As a healthcare professional, I’d like to add that the danger of transmission is greatest when caring for a sick person or in a healthcare setting that lacks sufficient infection control procedures.” (54 years old, male, Doctor and 56 years old, male, Stakeholder)
“A significant portion of the population became infected with the virus due to a lack of awareness and education regarding its transmission mode. I trust that our society is drawing valuable lessons from previous outbreaks to better prepare for the future, as transmission primarily occurs through close contact with bodily fluids.” (59 years old, male Stakeholder; 63 years old, male Stakeholder; and 56 years old, male, Doctor)
“I was told that EVD is transmitted to humans through the touch of fluids such as blood, vomit, feces, urine, semen, breast milk, saliva, and sweat of infected people, so I am just considering the message.” (46 years old, female, Nurse and 50 years old, male, Doctor)
“The Ebola virus is transmitted through direct contact with the bodily fluids of an infected person showing symptoms of the disease. Bodily fluids transmitting the virus include blood, saliva, sweat, semen, breast milk, urine, feces, vomit, and other secretions or excretions.” (53 years old, male, Doctor and 43 years old, male, Doctor)
“I have had the experience of coming in contact with an infected patient after the treatment process myself contracted. The virus can enter the body through broken skin or mucous membranes, such as the eyes, nose, or mouth. Once inside the body, the virus can cause severe illness and potentially death. We, the healthcare workers and those caring for infected individuals, are at higher risk of contracting the virus.” (58 years old, female, Nurse and 44 years old, male, Doctor)
“As a healthcare worker, I can confirm that the virus is transmitted through contact with infectious bodily fluids like blood, vomit, feces, semen, and more. Sharing needles or syringes contaminated with these fluids can also facilitate transmission. The most common way for someone to contract Ebola is by contacting an individual who is already infected. Therefore, it is paramount to exercise caution and avoid contact with potentially infectious fluids.” (52-year-old, female, Nurse and 57 years old, male, Doctor)
“Well, as we were told, and proven scientifically, EVD is primarily transmitted through direct contact with the bodily fluids of a person sick with EVD or who has died.” (45 years old, female, Nurse and 46 years old, male, Doctor)
“Yes, I know the virus is not airborne but transmitted through casual contact, such as touching or hugging an infected person. However, it is highly contagious, and people who come into close contact with an infected person are at high risk of contracting the disease. Healthcare workers and family members caring for an infected person are at risk of contracting EVD through direct contact with bodily fluids.” (60 years old, male, Doctor; 47 Years old, male, Stakeholder; 65 years old, male, Stakeholder)
“The virus spreads through sexual intercourse and can also be present in other bodily fluids during the later stages of the disease. As far as I know, direct contact with the body fluids of an infected individual can occur through various means, such as caring for the sick, handling contaminated objects or materials, or participating in burial rituals.” (51 years old, male, Doctor and 30 years old, female, Nurse)
Theme 2: Funeral attendance and EVD contraction
This theme is comprised of subthemes like traditional practices and crowded gatherings. Funeral attendance involves various activities, such as viewing the deceased’s body, offering condolences to the family, and participating in religious or cultural rituals that spread the virus rapidly. The participants’ quotes are as follows:
“From many health talks we have had over time, funeral attendance and burial rituals can pose a significant risk for the spread of EVD. During the 2013-2016 Ebola outbreak in West Africa, funerals were identified as a major transmission source, as people would come into close contact with infected bodies during traditional burial rituals, which often involve washing and kissing the deceased.” (43 years old, male, Doctor and 52 years old, female, Nurse)
“As far as I know, funeral attendance and burial rituals can increase the risk of EVD contraction because the virus can be present in the body fluids of infected individuals.” (30 years old, female, Nurse and 60 years old, male, Doctor)
“Over time, I have thought about funeral attendance and burial rituals that could increase the risk of EVD transmission, but I agree with the others.” (63 years, male, Stakeholder and 45 years, female, Nurse)
“Well, during the outbreak, our family members could not be buried correctly because of the spread of the virus. I am from Maryland County, and we love our traditional burial, but as a stakeholder in the Ministry of Health, I encourage people to stay away from dead bodies.” (59 years old, male, Stakeholder and 57 years old, male, Doctor)
“We, the stakeholders here at the Ministry of Health of Liberia, have identified funeral attendance and burial rituals as a risk factor for contracting EVD. However, it was difficult to avoid traditional activities like burial practices.” (56 years old, male, Stakeholder)
“We are now prepared to face any future outbreak because the Ebola outbreak has taught us a good lesson and exposed some prevention methods that can be implemented next time. During the Ebola outbreak, our people had no choice but to look at their loved ones go away without touching them.” (47 years old, male Stakeholder and 46 years old, male, Doctor)
“During the EVD outbreak, I went to a funeral for a friend who died from Ebola, and when I came back home the next day, I contracted the virus, but thankfully, I survived. Since then, I always tell people not to attend the funeral during the Ebola time.” (46 years old, female, Nurse and 51 years old, male, Doctor)
“Well, I did not contract the virus from funeral attendance and burial rituals, but some of my colleagues did, and as a medical doctor who survived EVD, the spread of the virus from funeral attendance is true. I hope we will be ready to control the virus in the future Ebola outbreak” (50 years old, male, Doctor and 58 years old, female, Nurse)
“Lofa County had the second-highest Ebola fatality rate, behind Montserrado County, because we, health stakeholders and healthcare workers, did not realize earlier that funeral traditions contributed to the high death rate.” (53 years old, male, Doctor)
“We still need more international help to prepare for future outbreaks because we do not have enough to spread awareness nationwide. Funeral activities are part of our people’s culture; we will need more international support to change that, like to spread more education.” (65 years old, male, Stakeholder and 56 years old, male, Doctor)
“Many Liberians are now concerned about burial arrangements in the event of any future epidemics, not just Ebola, and as a result, the situation will improve.” (54 Years old, male, Doctor and 44 Years old, male, Doctor)
Theme 3: Community-led prevention of EVD
This theme comprises surveillance, promoting good hygiene practices, increasing awareness, and contact tracing. Community-led prevention is highly recommended to improve local communities and raise awareness about the disease and its transmission. Community members working with local health authorities and other stakeholders should carry out these efforts. The participants’ quotes can be viewed as follows:
“We have implemented some community-led prevention programs to help carry out awareness around Liberia, which greatly helped control the virus.” (63 years old, male, Stakeholder and 43 years old, male, Doctor)
“Thanks for the question. It was not easy to organize those groups of people to spread the prevention measure news across the other counties in Liberia because those themselves were afraid of contracting the virus.” (60 years old, male Doctor and 57 years old, male Doctor)
“When I recovered from the sickness, I was among the first people in the Ministry of Health to lead community-led prevention programs in controlling the Ebola virus spread in Liberia from 2014 to 2016. There was more willingness to join the program in 2018 than 2014.” (59 years old, male, Stakeholder and 46 years old, male, Doctor)
“Because I was a member of those community-led groups, I can attest that community-led prevention efforts were crucial in reducing the spread of EVD in afflicted areas. These initiatives involve local communities in prevention and control activities, giving them the tools to play an active part in lowering the risk of transmission and protecting themselves and others from infection.” (51 years old, male, Doctor and 52 years old, female, Nurse)
“Yes, thank you for this interview. From the beginning of this program, the local community was skeptical about whether we were doing the right thing until the findings showed that hand sanitizer had been placed in a public place. These programs aimed to educate community members on Ebola virus transmission and prevention, as well as to promote good hygiene practices and encourage early reporting of suspected disease cases.” (50 years old, male, Doctor and 56 years old, male, Stakeholder)
“Community engagement and participation were critical during an outbreak for effectively preventing and controlling the disease. The implemented program included various activities, such as education and awareness campaigns, community surveillance and reporting, and promoting safe burial practices.” (58 years old, female, Nurse and 47 years old, male, Stakeholder)
“During the 2014-2016 Ebola outbreak in West Africa, I believe that community-led prevention programs played a crucial role in controlling the spread of the Ebola virus. I saw firsthand how these programs were instrumental in limiting the transmission of the virus by engaging local communities and empowering them to take action to prevent the spread of the disease.” (53 years old, male, Doctor and 65 years old, male, Stakeholder)
“Based on what I have observed, community-led prevention programs demonstrate a high level of effectiveness in managing the Ebola virus transmission. These programs are intentionally structured to actively involve and empower local communities in preventing and controlling disease outbreaks.” (46 years old, female, Nurse and 56 years old, male, Doctor)
“Well, some of the community-led programs we had put in place are now vanishing from the program checklist we implemented, but I hope we put everything back on track.” (45 years old, female Nurse and 54 years old, male Doctor)
“The past outbreak surprised us, so the effort was not applied until late 2016. The community-led program started almost at the outbreak’s end but helped tremendously.” (44 years old, male, Doctor and 30 years old, female, Nurse)
Theme 4: Ebola virus vaccine concern
This theme comprised subthemes like a false sense of security, limited data, and potential side effects. A combination of research is required to tackle the lack of vaccines in Liberia and their effectiveness. Several experimental Ebola virus vaccines have been developed in recent years, including the rVSV-ZEBOV vaccine, which was shown to be highly effective in clinical trials during the 2014-2016 West Africa Ebola virus outbreak. The participants’ quotes are in the following:
“As a health worker, I find waiting to receive the vaccine frustrating. I did receive much support when I fell ill with the Ebola virus and was admitted to the hospital. Throughout the outbreak, I overheard discussions about developing an Ebola vaccine designed to reduce the risk of infection and assist in managing disease outbreaks.” (52-year-old, female, Nurse and 43 years old, male, Doctor)
I chose not to receive the Ebola vaccine because I was informed about its common side effects, including pain, redness, swelling at the injection site, fatigue, headache, muscle pain, and fever.” (58 years old, Female, Nurse and 60 years old, male, Doctor)
“Some individuals may have concerns about the safety and effectiveness of the Ebola vaccine, as it is a relatively new vaccine that has yet to be extensively studied. As a stakeholder in the Ministry of Health, I am supposed to have all the answers, but I do not.” (47 years old, male, Stakeholder and 57 years old, male, Doctor)
“Well, we hoped to receive the vaccine in Nimba County, but it did not reach there. Even if the vaccine were to arrive in Nimba County, I do not think I could take it because of fear.” (46 years old, female, Nurse and 46 years old, male, Doctor)
“The Liberian government failed to give sufficient proof to persuade citizens to take the vaccine.” (51 years old, male, Doctor and 45 years old, female, Nurse)
“Due to a lack of clear education about the Ebola virus vaccine, I found it challenging to decide whether to take it. Most resources and assistance were concentrated throughout the Ebola outbreak in Monrovia, the capital city. For instance, people in Maryland county did not receive adequate support.” (50 years old, male, Doctor and 53 years old, male, Doctor)
“The international community did not adequately address concerns about the vaccine’s effectiveness, leading to doubts among many people, including myself. I apologize, but I chose not to take it for personal reasons.” (56 years old, male, Stakeholder)
“Before distributing the vaccine to the public, conducting a comprehensive public education campaign is essential to inform people about its effects. I played a role in the vaccine committee, and it’s worth mentioning that a significant number of individuals declined to receive it.” (56 years old, male, Doctor and 30 years old, female, Nurse)
“I am sorry I did not take the vaccine; I do not know my clear reason. I guess I just follow people’s concerns.” (54 years old, male, Doctor and 44 years old, male, Doctor)
“We need more vaccine research. We, the Liberians, must be among the best scientists out there to be unable to decide what to provide to our people. I was apprehensive about the safety of the Ebola vaccine.” (59 years old, male, Stakeholder and 65 years old, male, Stakeholder)
“I am presently formulating a proposal for the establishment of a clinical trials laboratory to be situated in Monrovia. This facility will be crucial in advancing our understanding of vaccine manufacturing processes.” (63 years old, male, Stakeholder)
Theme 5: Challenges in implementing prevention measures for EVD outbreaks
This theme is comprised of subthemes like inadequate health infrastructures, difficulty tracing infected people, lack of resources, and cultural and social barriers. The healthcare barriers have been the grassroots conversation about the EVD outbreak in Liberia. One of the significant barriers is that the government is paying less attention to improving the healthcare system in Liberia. The participants’ quotes can be seen in the following:
“As I know, the challenges connected to the EVD outbreak have to do with the misunderstandings and mistrust of health workers, response efforts, and the disease can create barriers to implementing prevention measures.” (43 years old, male, Doctor and 52 years old, female, Nurse)
“Misinformation about the disease and its transmission can also lead to fear and resistance to prevention measures.” (58 years old, female, Nurse and 60 years old, male, Doctor)
“Yes, I can tell you that Liberia has a significant economic problem, and the economic impact of the Ebola outbreak made it more difficult to contain the outbreaks.” (63 years old, male, Stakeholder and 59 years old, male, Stakeholder)
“Our public health infrastructure must be strengthened in high-risk areas to quickly detect and respond to possible outbreaks. This was a major obstacle during the Ebola outbreak, resulting in many deaths.” (46 years old, female, Nurse and 57 years old, male, Doctor)
“I can attest to the stigma issue because I faced that myself when I recovered from the virus. People suspected or confirmed to have Ebola may face discrimination and rejection by their communities, making it difficult to access health care and other essential services.” (46 years old, male, Doctor and 51 years old, male, Doctor)
“As a healthcare worker, I have to be clear that Liberia’s health system is weak, including the rest of the counties around Liberia. This can make it difficult for healthcare providers to effectively implement prevention measures and provide appropriate care for infected people.” (50 years old, male, Doctor and 45 years old, female, Nurse)
“We never had accurate data collection and surveillance methods, which are critical for tracking and responding to the Ebola virus outbreaks, and it was also challenging in resource-constrained settings.” (53 years old, male, Doctor and 30 years old, female Nurse)
“The resistance to change is a big issue because some individuals and communities may resist change and be reluctant to adopt prevention measures, such as wearing personal protective equipment or practicing good hygiene.” (56 years old male, Stakeholder and 56 years old, male, Doctor)
“The government mistrust between communities and health authorities was a significant challenge during the 2014-2016 Ebola outbreak and remains a challenge. Community mistrust can hinder efforts to implement effective prevention measures, such as community-based surveillance and contact tracing.” (54 years old, male, Doctor and 47 years old, male, Stakeholder)
“I want to say that the lack of health policy making has brought more challenges to implementing prevention measures, such as trained healthcare workers, community health workers, and outbreak response teams. More policymaking needs to be implemented to improve the next outbreak.” (65 years old, male, Stakeholder and 44 years old, male, Doctor)
Theme 6: Liberia’s health systems
This theme comprises subthemes like weak and underfunded, fragile health infrastructure, and inadequately provided health facilities. A better healthcare system is needed to strengthen its standards as it opens the gateway to improving healthcare services across Liberia. The strengthening has to include health policies, institutions promoting health-related infrastructure, laboratories, medical equipment, pharmaceuticals, public health programs, and health financing mechanisms. The participants’ quotes are as follows:
“Well, looking at the health system in Liberia, it is considered weak and underfunded. My community was deprived of reasonable health assistance compared to the other counties. In New Kru Town, we are not receiving enough medical aid to fight the Ebola virus in the long run.” (43 years old, male, Doctor and 60 years old, male, Doctor)
“Well, I will say first that the health system in Liberia is still recovering from the impact of a long-standing civil war and the 2014-2016 EVD outbreak, which had a devastating effect on the country’s fragile health infrastructure. As a result, access to basic health services and resources is limited, and many health indicators remain among the lowest in the world.” (63 years old, male, Stakeholder; 57 years old, male, Doctor)
“We know that Liberia’s healthcare system encounters substantial difficulties, especially in rural regions where access to health services is restricted. Even in the area where we are currently operating, obtaining the necessary clinical materials can be quite challenging.” (46 years old, male, Doctor; 52 years old, female, Nurse)
“Liberia is a low-income country with significant healthcare challenges, but we do as much as possible to fix the issue. I have noticed that everything about improved healthcare is located in Monrovia’s capital, so I want to change that.” (58 years old, female, Nurse and 51 years old, male, Doctor)
“Despite my involvement as a stakeholder, it is undeniable that Liberia’s healthcare system has confronted numerous hurdles in recent years. These difficulties include financial resources, insufficient staffing, healthcare worker training, and restricted access to medical material and advanced technology. Additionally, the country endured a devastating Ebola outbreak from 2014 to 2016, which served as a stark reminder of the inherent weaknesses and vulnerabilities within the healthcare system.” (59 years old, male, Stakeholder, and 56 years old, Stakeholder)
“The Ebola outbreak from 2014 to 2016 placed additional pressure on the healthcare system, shedding light on deficiencies in infrastructure, personnel, and resources. Subsequent endeavors have been undertaken to enhance Liberia’s healthcare system, encompassing investments in healthcare infrastructure and workforce enhancement. Moreover, initiatives have been launched to enhance access to vital medications and healthcare services.” (50 years old, male, Doctor and 46 years old, female, Nurse)
“Well, as for my community, there were no good facilities; however, the quality and availability of healthcare services in Liberia can vary depending on the location and resources available. In recent years, Liberia has made efforts to improve its healthcare system, including investments in healthcare infrastructure and training for healthcare workers.” (53 years old, male, Doctor and 45 years old, female, Nurse)
“Working as a healthcare professional is challenging due to the country’s predicament. Many people in these places rely on self-medication, which can lead to major health consequences. The government has attempted to strengthen the healthcare system by boosting healthcare funding and investing in medical professional training. I am sure we can fix everything from now to 2035 as we plan our vision.” (47 years old, male, Stakeholder and 65 years old, male, Stakeholder)
“I did want to emphasize that we require support. The healthcare system in Liberia has major obstacles, including a lack of educated healthcare personnel, insufficient facilities and equipment, limited access to essential medications and supplies, and a shaky health finance system. Many hospitals are understaffed and lack basic equipment and supplies, such as drugs and diagnostic tools.” (56 years old, male, Doctor and 54 years old, male, Doctor)
“Liberia has a high burden of infectious diseases, including EVD, and there are significant gaps in access to healthcare services, particularly in rural areas.” (30 years old, female, Nurse and 44 years old, male, Doctor)
Discussion
The study aimed to explore the EVD’s potential risk components, prevention measures, and lessons learned during the outbreak in Liberia. The participants’ answers and opinions that formed themes are discussed in the following:
Theme 1, “Mode of transmission,” indicated that the participants agreed that the Ebola virus is most commonly transmitted through direct contact with an infected person’s bodily fluids, such as blood, sweat, urine, sperm, vaginal secretions, and breast milk. The virus can also be contracted through unprotected sexual contact or contact with contaminated surfaces or needles. Furthermore, we emphasized that the risk of transmission is greatest when caring for a sick person or in a healthcare facility that lacks effective infection control measures. To reduce the risk of transmission, infection control measures such as wearing personal protective equipment, practicing good personal hygiene, and avoiding direct contact with an infected person’s bodily fluids are all recommended. On the other hand, those who saw the illness as normal were aware that it was dangerous and contagious.
Similar to the current study’s findings, Akbarialiabad et al. (2022) discovered that mistrust of government or public health officials, as well as concerns about the spread of disease from healthcare facilities, were obstacles to healthcare-seeking behavior, early diagnosis, and timely disease prevention and control treatment. EVD can be passed from one person to another through bodily fluid contact with a sick or deceased person (International Ebola Response Team et al., 2016). According to Appiah-Sakyi et al. (2021), sexual transmission of the Ebola virus is possible.
Theme 2, “Funeral Attendance,” indicated that the participants believed that Liberians’ customary funeral and burial practices held religious and cultural significance. Physical contact with the deceased was kept until their burial before the Ebola pandemic (Bebell et al., 2017). Culturally influenced improper burial rituals underwent a dramatic change during the 2014–2016 EVD outbreak, with hardly any traditional religious or cultural practices being observed. At the Ebola burial site, Muslims, Christians, and people of other faiths were interred together. Family members were forbidden to go to the cemetery (Fallah et al., 2016).
Theme 3, “Community-led prevention of EVD,” highlights that the members of the Liberian community were more willing in 2018 to return to prevention measures quickly than in 2014-2016. This finding suggests that, despite some dissatisfaction with the government and public health officials, people realized that the government interventions, perceived by the community as a harsh approach to ensuring safe healthcare in Liberia, were not as bad as they appeared. Consequently, the shared objective was to guarantee sufficient community involvement and outreach for continuous EVD monitoring, health instruction, and a dedication to delivering safer healthcare that is respectable and acceptable to every Liberian community. The current progress in community-led-prevention EVD knowledge transfer was reported by Abo (2020). This progress is bolstered by the continuous efforts of public health teams and community leaders to work together to provide community engagement.
Theme 4, “Ebola virus vaccine concern,” indicated that some people in Liberia still await the vaccine. When they were sick with the Ebola virus and admitted to the hospital, they did not receive the vaccine. According to the WHO Ebola Response Team (2014), the purpose of the Ebola vaccine was to lessen the likelihood of contracting the virus and aid in the containment of disease outbreaks. Nevertheless, there is no proof that the vaccination lowers the risk of infection. A previous study by Agnandji and Loembe (2022) pointed out that taking the Ebola vaccine may include potential side effects, limited data on the vaccine’s long-term safety, and the possibility of developing a false sense of security and not following recommended infection control measures.
Theme 5, “Challenges in implementing prevention measures,” underlined that the majority of informants mentioned a lack of funding, poor health infrastructures, trouble finding infected individuals, and social and cultural barriers. The grassroots discussion about the Ebola virus outbreak in Liberia has created barriers to healthcare. The government’s lack of focus on high-quality healthcare is one of the major obstacles. WHO Ebola Response Team (2014) reported substantial challenges for generalists in healthcare working in Liberia. Recognizing that Ebola survivors have already been through a difficult and traumatic experience is critical. Discrimination exacerbates their suffering and makes reintegration into society more difficult. In the aftermath of an Ebola outbreak, efforts to combat discrimination and promote understanding are critical.
Theme 6, “Liberia’s health systems,” indicated that Liberia’s healthcare facilities, with a poorly trained medical team, are underequipped and understaffed. Most medical personnel in various healthcare settings are undertrained (Arthur et al., 2023; Arthur, 2002). Regrettably, the global public health community came too late, as the epidemic spread swiftly and the death toll shot through the roof. Public health officials did everything in their power to address the needs of the public, but they were either unable or did not have the resources to halt the disease’s spread completely. Healthcare professionals, community leaders, and legislators chastised global health programs because there was no recognized remedy or documented mechanism or strategy for controlling the ailment (Akbarialiabad et al., 2022). As fatalities increased, panic spread throughout the community as their ignorance of the unknown disease that killed people increased and instilled fear. Other researchers who had previously conducted EVD-related tests acknowledged a problem with a lack of resources (Lévy et al., 2018; Malik et al., 2023).
Implications of the Study
This study is essential for nurses, particularly community health nurses, because the implications of EVD for nursing cover a wide range of responsibilities, from direct patient care to education, surveillance, and research. Nurses play an essential role in effectively managing and controlling the spread of EVD while also providing compassionate care to those affected.
The EVD remains a global fear regarding the lethal nature of EVD, and the possibility of another outbreak still exists. Countries with poor socioeconomic positions, poverty, inadequate infrastructure, and medical professionals and equipment shortages were unprepared. As Liberia is one of these unprepared nations, we aimed to comprehend the associated potential risk components and mechanism of EVD transmission among Liberians during the past epidemic. This study could add to the corpus of information already available to support stakeholders and policymakers in making decisions. According to this study, washing the dead bodies of Ebola victims, touching the body and bodily fluids, kissing the body, wearing the deceased’s contaminated clothing, not washing your hands, and human-to-human contact were all possible risk components contributing to the transmission of EVD. It has been difficult for medical professionals to contain EVD outbreaks.
Thematic analysis techniques are useful for articulating and characterizing the themes that have been identified based on the potential risk components, including personal belief systems and cues to take action or remain inactive. Participants’ perceptions of susceptibility to the EVD outbreak were used in this study. Participants enrolled in this study were stakeholders and health service providers. As a result, the comprehensive knowledge gathered can be used for public health preparedness; multidisciplinary teams such as health professionals, communities, researchers, and government officials together to avoid and limit future outbreaks.
Studying patient satisfaction offers valuable insights for enhancing healthcare training across various nursing practice domains. In this study, all our participants were stakeholders and healthcare professionals with experience contracting EVD. The comprehensive knowledge derived from this study can empower nurses, doctors, stakeholders, and multidisciplinary teams to collaboratively elevate healthcare quality on both national and international levels. The findings of this study might contribute to changing dangerous habits and increasing public health awareness. Health education and literacy initiatives, policy implementation, and individual and group decision-making can bring social change. As global health practitioners engage with the government of Liberia to develop disease prevention policies and plans for future infectious disease outbreaks, this study can provide essential elements and reliable information needed to support healthcare policies and nursing practice.
Strengths and Limitations of the Study
This is the first study exploring the lived insight of stakeholders and health workers, including nurses in Montsrrado County. Only 20 participants who had recovered from EVD met the study’s eligibility criteria. Despite several participants providing similar responses and reaching data saturation, we are confident that the experiences shared by participants are similar to those of other research. Another potential limitation of our study is the selection process. Purposive sampling was used to select participants. While this process could have resulted in selection bias, it was also the foundation for establishing trust and openness. Alternatively, because of our close relationship with the community, social desirability bias could have influenced some participants’ responses. However, Sandelowski (2000) stated that purposeful sampling was the most appropriate strategy for descriptive qualitative research and that sampling should allow the researcher to capture and describe the phenomena over various situations. Lastly, recall bias may exist when asking participants about their experiences during the Ebola outbreak; that being said, we think the information is fairly trustworthy because every participant had personal experience with EVD and also worked as a nurse and medical practitioner. Notwithstanding these drawbacks, we believe the results of this study can contribute to the critical body of knowledge regarding possible risk components and EVD prevention measures.
Conclusion
This study explored the potential risk components and prevention methods of EVD. The data were gathered from healthcare workers and health stakeholders with scientific competencies exposed to the disease during the EVD outbreak. They said the potential risk components included contact with a sick or dead person’s bodily fluid, sexual intercourse with a sick person, and traditional burial. Funeral attendance gave subdivision to traditional practices and crowded gatherings. Some critical challenges and opportunities related to the Ebola outbreak in Liberia were identified and discussed. Community-led prevention promotes good hygiene practices, increasing awareness, surveillance, and contact tracing. Some participants were still waiting for the Ebola vaccine; however, some had a false sense of security, limited data, and potential side effects of the vaccine. The challenges in implementing prevention measures included inadequate health infrastructures, difficulty tracing infected people, lack of resources, and cultural barriers. Liberia’s health systems gave branches to weak, underfunded, fragile health infrastructure and inadequately provided health facilities.
Several potential risk components contributing to the EVD outbreak should be a public concern. Strengthening the current healthcare system supported by local community and international aid providers (multidisciplinary teams) is needed to anticipate the behavioral problem and improve the efficacy of the prevention measures appropriate to the conditions in Liberia. The findings of this study underscore the significance of strict adherence to infection prevention and control measures. Nurses might need to be vigilant in following recommended practices such as proper hand hygiene, the use of personal protective equipment, and isolation procedures. The results of this study can help inform future intervention strategies for EVD.