










Pulmonary Tuberculosis (TB) is a serious health care problem associated with mortality as a top ten worldwide death (World Health Organization, 2019). According to World Health Organization (WHO), the number of global cases is around ten million, and more than one million people die every year (World Health Organization, 2019). Besides, the number of new incidences increases by two to three million annually (Imsanguan et al., 2020). From statistics, Thailand is one of the 14 worst countries having the highest burden of tuberculosis, human immunodeficiency virus (HIV), and multiple drug-resistant cases (MDR) spreading across the country rapidly (Johnston et al., 2009). However, WHO communicates a universal strategy for reducing the prevalence of pulmonary TB cases to be less than 10 per 100,000 population by 2034. Additionally, Directly Observed Therapy, Short-course (DOTS), is recommended as a critical element for the cure and prevention of TB (Ahmad et al., 2018; World Health Organization, 2019).
The DOTS is the policy package for TB control in order to achieve drug adherence (Gyimah & Dako-Gyeke, 2019; Tadesse, 2016). Thailand is challenging the high prevalence of lower cure rate and non-adherence to TB drugs regarding drug adverse, barrier of access to healthcare, lack of knowledge, and psychological distress (Tadesse et al., 2013). Consequently, a significant barrier to TB control is related to the non-adherence to TB drugs (Choowong et al., 2019; Gugssa et al., 2017; Imsanguan et al., 2020). To be consistent with taking the TB drug by family, the health profession should systematically monitor and ensure that TB patients will take the drug (Brown et al., 2015). Recent studies show that those who had first TB diagnosis would perceive the experience of stigma as leading to hiding their illness and impact on the consists of adherence to the drug (Brown et al., 2015; Tadesse, 2016). Also, the burden of treatment can be the workload of health personnel to conduct DOTS and barriers to access health facilities as TB patients need to receive DOTS every day (Dias et al., 2013).
The Thai national guideline recommends choosing the family member to monitor the drug taken in TB patients to promote drug adherence (Choowong et al., 2019). Currently, Thailand's structure has changed from expanding to single-family; inevitably, it is difficult to monitor (Yu et al., 2018). Therefore, focusing on poor compliance and barrier to self-care in TB reveals that well-being is a barrier to encouraging TB adherence to drugs (Brown et al., 2015). Furthermore, pulmonary TB is a chronic illness, and TB patients suffer from long-term treatment as the burden of disease (Tadesse et al., 2013). In addition, TB patients experience psychological distress such as stigma, anxiety, or depression as transferred to physical health (Brown et al., 2015; Tadesse, 2016).
However, TB patients perceive the burden of diseases such as lack of social support to reach the DOTS, resource facility, or cost of treatment led to halting continuing care and loss of follow-up (Brown et al., 2015; Tadesse, 2016). Those are considered several factors leading to the burden of disease and obstacles to treatment for TB (Gyimah & Dako-Gyeke, 2019; Tadesse, 2016). Therefore, this study aimed to explore patients' perceptions regarding their experience in the DOTS treatment, which may inform the burden of the disease and improve TB health care in continuum care.
Methods
Study Design and Setting
A qualitative descriptive approach was used to explore patients' experiences living with pulmonary TB. The research was conducted in a slum community in Bangkok, Thailand.
Participants
Twenty participants were selected using convenience sampling. The inclusion criteria of the participants were (1) those who were diagnosed with pulmonary TB and (2) who received the DOTS treatment.
Data Collection
Data were collected from April 2018 to December 2018. In this study, the researchers worked together with community nurses for the data collection process. First, the participants who met the inclusion criteria were invited to participate. Then, once they agreed, the researchers and nurses asked the participants for a convenient interview date and time.
The data were collected using semi-structured interviews. Each interview was audio-recorded and lasted for 30-90 minutes. The questions were developed based on findings from a previous study of the burden of disease among TB patients (Gyimah & Dako-Gyeke, 2019). Hence, the example of the questions such as: “How do you live with TB?”, "How do you experience the burden of disease?", “How about your treatment with DOTS?” and continued following the answers from the participants. The interview was conducted using the Thai language, and it was stopped until the researchers heard the same information repeatedly.
Data Analysis
The audiotapes were transcribed verbatim by the first author after checking for accuracy by comparison with the audio recordings. The interview transcripts were read twice and compared recording by two authors (AK and WS) several times to obtain a comprehensive perspective on the content and ensure accuracy. The meaning was categorized, and codes were addressed, modified, and merged, if necessary, by referring to cluster and individual aspects.
The two authors analyzed the interviews in parallel separately. Then, results were discussed together to reach an agreement on themes and subthemes. The Thai language was used for interviews and coding, and the English language was used in data analysis and manuscript writing. In addition, transcripts were made anonymized and were available for the researchers only. The participants' quotes were carefully translated from Thai to English by a researcher proficient in both languages. The primary goals of the translation are to maintain the meaningful content of the quote and preserve the patients' voices. Additionally, the thematic analysis outlined by Saks and Allsop (2012) was used to manage the data and enable a more systematic analytical approach to obtain an overview and identify themes and subthemes.
Rigor
To ensure the rigor of the data collection, all interviews were conducted by using a semi-interview guide. AK conducted all the interviews to ensure data saturation. Three authors (AK, WS, and KP) were involved in all data analysis steps, independently reread the interviews, discussed the findings, and developed codes and themes.
Ethical Consideration
The study was approved by the Research Ethics Committee of Suan Sunandha Rajabhat University, Thailand (No. COA 1-026/2018) and complied with the principles laid down in the Declaration of Helsinki. Prior to the study, the researchers explained the purpose and the procedures of this study to participants. All participants have signed informed consent before enrollment, and they could withdraw from the study at any time without any penalty.
During the interviews, some participants had an emotional feeling and were sensitive while talking about some of the themes pertaining to their stigma moment. Therefore, the interview was paused to calm them down then resumed with their permission, or the participants could take a break or reschedule the interviews.
Results
Characteristics of the Participants
This study consisted of 20 patients with pulmonary TB treatment, divided into 15 males and five females, with ages ranging from 20 to 56 years old. Most patients had the DOTS experience at least six months (n = 15).
Thematic Findings
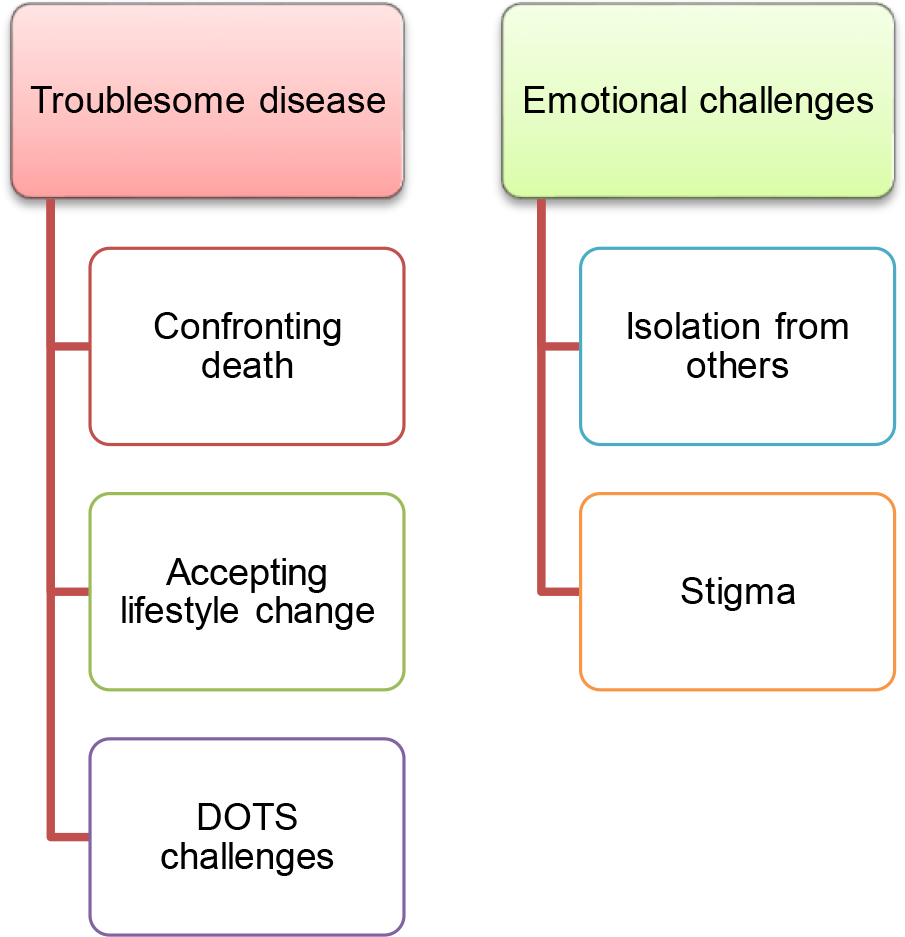
Two themes were developed in this study: (1) Troublesome disease and (2) Emotional challenges (see Figure 1). Each theme has subthemes described with the following quotes from the participants.
Theme 1: Troublesome disease
Most participants expressed their perception of being extremely agonized from several symptoms, thereby making them feel close to death. The first main theme describes the experience of troublesome diseases consisting of three subthemes; (1) confronting death, (2) accepting lifestyle change, and (3) DOTS challenges.
Subtheme 1.1: Confronting death
Most participants stated as they visited a door of death that they experienced extreme agonizing and suffering from several symptoms, such as severe coughing and difficulty breathing. They were unrealized to the worsening symptoms until they perceived extreme pain and agonized and required hospitalization.
"I was so tired as I nearly died. It was difficult to explain how I was tired as it was so difficult to breathe as I received less oxygen. Sometimes, it was so agonized while I was breathing to pull up-down with my chest as my chest was so heavy. I felt like something heavy pressed on my chest making me difficult to breathe as an elephant sitting on the chest." (ID1)
"When it was flared-up as it was difficult to breathe as I nearly die. I have never been like this before as I could not breathe well." (ID6)
Consequently, participants experienced extremely painful and agonized various symptoms of the TB disease. Furthermore, their limited understanding of the nature of TB disease thereby led them inadequately prepared for recognizing and responding to the acute episode of TB disease.
Subtheme 1.2: Accepting lifestyle change
Several participants stated that their lifestyles had changed since being diagnosed with TB disease. They expressed their need to adhere to medications to cure the disease. In addition, their daily physical performances have been changed by disease's progressive as they are tired easily compared to before.
"My life has changed since I have TB disease, and I need to take almost ten tablets per day. I never took tablets as much as this before. So, I have no choice because what helps me to get better is the medication." (ID12)
"My life has changed since I have got this disease. So, I could not work or even walk or talk as before because I was tired easily. So, I have to do everything slowly or take a break or sit down if I feel tired." (ID4)
As a result, participants accepted the lifestyles change to the new situations affecting the medication adherence and adjusting their physical activities to new norm living rather than those who are unaccepted the new norm life.
Subtheme 1.3: DOTS challenges
Most participants expressed their concerns about supports from their families to continue the DOTS treatment. Although they confronted challenges with side effects of the TB medications, they also received strong support from their families that could help them continue complying with the TB medications.
“It is great to have someone to remind you about time for medications, to ensure you won't forget" (ID3)
"At first, I could not believe that I had got TB diagnosis as I denied the disease and treatment. So, my mum encouraged me to follow the DOTS treatment. She always monitors while I take the medicines. It is great to have someone to remind me time for the medications, to ensure that I do not forget to take it."
"I have been following the DOTS for nearly two weeks, and my wife always monitors me. I have several side effects such as weight loss, nausea, loss of taste. Sometimes, I feel that my body cannot tolerate the side effects anymore, and I want to stop taking it, but my wife encourages me to take it. It is good to have family supports and encouragement to take these medications." (ID15)
As a result, participants stated that they received support monitoring the DOTS from their intimate and family. Some participants suffered from side effects of the medications, thereby making them discontinue the DOTS.
Theme 2: Emotional challenges
Several participants experienced a negative emotional by being diagnosed with TB. Most of them described that they were isolated from family and society. The second theme addresses the emotional challenges, which are (1) isolation from others and (2) stigma.
Subtheme 2.1: Isolation from others
Participants explained that they experienced negative feelings about having TB due to their limited understanding of the disease, which led to bad emotions, such as loneliness, fear, or shame. They also expressed that they isolated themselves from others because they did not want others to have the disease.
"I use a scarf as a mask because I do not want to use a mask because people will think that I'm sick with the awful disease. So, I separate everything such as a cup, dish, spoon, and towel from everyone at work or even my family because I do not want them to get the disgusting disease from me." (ID5)
"I do not sit in a public because I'm too scared that I'm a cross-infection of TB. So, I sit separately from others, even my family." (P11)
Most participants perceived that they were cross of infections to others easily caused by the misunderstanding concepts of TB disease.
Subtheme 2.2: Stigma
Most participants experienced being diagnosed with TB as it is repulsive in society due to their lack of knowledge of the TB disease. Also, Thai people believe in a traditional culture that being diagnosed with TB is one of the diseases ignored by society. Their perception of stigma thereby leads them to emotional distress, such as stress and hopelessness.
"It is so sad having TB diagnosed. I heard that TB is one of the diseases that the whole world disgusts. I'm so scared that the disease could not be the cure." (ID13)
"Once I have been diagnosed with TB pulmonary, the whole world stops moving, why it happens to me. I feel stressful. I have never been out drinking or smoking, so I have a lot of questions for myself. Of course, I do not want to tell anyone that I have been diagnosed with TB. I am afraid that others will feel scared and disgusted with me. So, I will keep it a secret until I die." (ID6)
Consequently, participants experienced a perception of sigma due to the misunderstood nature of TB disease. In addition, their cultural beliefs also influence negative emotions leading them to decide to hide the disease.
Discussion
This study demonstrates the consequence of the actual experience of patients with pulmonary TB receiving the DOTS treatment. They challenge troublesome disease and emotional challenges (Yu et al., 2018). This study also explores experience with TB pulmonary to promote the optimal health care for the success of the DOTS treatment (Brown et al., 2015; Dodor, 2012).
The findings indicate that participants’ perceptions of troublesome disease are extremely painful from several symptoms, as they expressed, close to death. In addition, most participants stated that they perceive emotional distress such as depression, stigma, or isolation as they recognize that it is a disgusting disease by their limited understanding of TB disease.
As participants suffer from various symptoms such as the difficulty of breathing, exhausted and limited physical activities. They are also highly agonized in active phases as they cannot breathe efficiently as they get closer to dying. In addition, they also perceive that the disease impacts their daily living (Brown et al., 2015). However, those realized lifestyle changes seem to cope with strategies successfully, adapt to a new norm, and comply with treatment rather than those uncertain about their illness (Orenstein et al., 2009). A few participants stated that they have trouble with medicine as they could not tolerate the side effects of TB medications, leading them to discontinue the DOTS treatment and rely on their severity of side effects (Culqui et al., 2012).
The result also found that most participants perceive emotional distress caused by a reaction from the communities or society, making them have stigma having cross infections into others. Most participants also stated that they perceive isolation from others—the psychological distress impacts continuing compliance with the DOTS treatment. The unjust treatment might indicate the needs of patients as well as the holistic care approach.
The emotion of stigma could decrease the ability to perform daily physical living and the adherence to prescriptions (Choowong et al., 2019). Participants stated that they have stigma caused by the cross-infections to their intimate or society. As a result, they experience overwhelmingly troubling disease and treatment, side effects of TB drugs, and emotional distress. However, the cultural belief becomes a part of their lives and influences how they cope with strategies and manage the disease (Orenstein et al., 2009). Most participants learn from previous experiences that TB is diagnosed as a disgusting disease leading them to hide their condition (Getahun et al., 2016). The emotional issue is an essential aspect of living with TB regarding patients' adherence, well-being, and quality of life (Bastos et al., 2017). Besides, healthcare professionals should be concerned with patients' emotional aspects and pay more attention to their individual needs in order to improve their quality of life and well-being (Kim et al., 2009).
In addition, nurses and multidisciplinary teams should be concerned about the perception of individual patients' experiences to enhance the consistency of the DOTS treatment (Kigozi et al., 2017). Therefore, nurses play an essential role in the multidisciplinary team to implement and develop the educational program guidelines to promote medication compliance in terms of individual needs.
Further study should examine the implementation of adherence treatment, psychological support, and patient educator to promote and enhance treatment compliance. The limitations of this study are challenging to find the eligible participants. Some patients conceal their illness and find it difficult to find the available and suitable location for interviews.
However, this study provides new knowledge, although it was conducted in 2018. Nevertheless, the findings are still significant in the current situation because TB is still a big issue in Thai society. Therefore, health professionals, including nurses, need to pay attention to the DOTS strategy.
Conclusion
The inner voice of TB patients is important information for healthcare professionals in order to improve the DOTS strategy. The current study found that patients with TB are overwhelmed by troublesome disease and treatment and suffer from negative emotions such as stigma and feeling isolated from others. In addition, TB patients perceive physical and mental health problems leading them to discontinue the DOTS treatment due to their insufficient knowledge of TB disease. Therefore, nurses and healthcare professionals should develop an educational program that includes psychological aspects based on individual needs to improve the holistic approach.