









Background
The recovery from illness and safety from adverse events or preventable complications during the medical process is the expectation of the patients and reflects the quality of patient care. Nurses play an essential role in managing risks and protecting patients, and nursing practice must be based on safety principles and do not cause any harm or risk to patients (World Health Organization, 2011). Nursing organizations, therefore, place importance on patient safety by defining them as part of competencies in nursing practice. It also deals with issues of ethics and professional law. Nevertheless, the errors in patient care leading to adverse events are mostly preventable (World Health Organization, 2011).
Patient harm in healthcare facilities is the leading cause of morbidity and mortality internationally that affects the significant outcomes of patient care, cost burden, and health care system (Pangh et al., 2019). In Thailand, patient safety is integrated into the quality development process and set as one of the criteria for quality assurance in hospitals, which must be the first awareness of the medical personnel (Yoelao et al., 2014). Therefore, it is essential for health care education to focus on the importance of healthcare professionals to have a foundation in knowledge, skill, behavior, and attitude relevant to patient safety in all actions (Tella et al., 2014).
In terms of the nursing context, patient safety problems are related to human factors and work processes, such as infection control procedures, medication errors, infection control procedures, medication errors, and communication failure. Therefore, raising awareness requires the development of a safe patient care management system and the human factor related to individual nurses due to the high workload, negligence, lack of knowledge or skill, and miscommunication (Tella et al., 2014; Yetti et al., 2021). Thus, the cultivation of patient safety in nursing students must be from nursing theory and learning from experiences in nursing practice. These will shape nursing students to keep patient safety in mind and make it a part of normal behavior. According to the study of Bandansin et al. (2020), the patient safety awareness competency of nursing students refers to students protecting patients or reducing the likelihood of injury, complications, or adverse events due to limitations in terms of knowledge, skills, lack of harm prevention, neglect and making a mistake. Additionally, nursing students’ patient safety awareness competency consists of two components: (1) management to ensure patient safety and (2) solving the hazard problem in patient care. However, nursing students, the future professional nurses, must participate with the healthcare team in reducing or eliminating the risk of harm to patients (Lee et al., 2014; Usher et al., 2017).
Developing nursing students into professional nurses with competence in patient safety awareness will help them recognize the potential risks of the cognitive misunderstandings that lead to medical care errors. However, this competence is achieved by focusing on managing learning experiences in classrooms and clinics to foster awareness of patient safety care. Literature review indicated that applying the Metacognitive Experiential Learning Model to design the learning processes establishes a body of knowledge from learners’ own experiences and practice (Kolb & Kolb, 2009; Tanaka et al., 2016). Therefore, this model is appropriate for patient safety practice by using questioning to inquire about nursing problems that could be solved rationally. In addition, questioning encourages thought, linking experiences with theoretical knowledge, monitoring and controlling their cognition, behavior, and problem-solving during operations to achieve the targeted results (Torabizadeh et al., 2018).
Questioning is a tool for students to develop higher-order thinking skills and desirable attributes. Higher cognitive questioning is conducted to achieve a deep awareness and a reflection of what will be done, such as carefully understanding the role, responsibility, and appreciation of the value of nursing practice (Lakdizaji et al., 2013). In addition, the integration of patient safety into clinical practice bridges the traditional learning gap that lacks a connection of the theoretical knowledge learned in the classroom and the real world by teaching risk-based thinking to emphasize situational awareness and learning from errors (Fore & Sculli, 2013).
In this study, the clinical learning model is developed to enhance patient safety awareness competency among nursing students, which applied metacognitive thinking through experiential learning (using a questioning strategy as a tool for patient safety learning, which the learners think critically and question their experiences related to the safety of nursing activities with patients) and reflective learning (the teacher's questions encourage the nursing students to criticize the experience associated with the patient hazard, near miss situations to improve their doing in other conditions). This clinical learning model aims to enhance patient safety awareness among nursing students to build a culture of quality and safety in nursing practice.
Methods
Study Design
A research and development approach was used in this study, with two phases: First, developing a clinical learning model to enhance patient safety awareness competency among nursing students, which was conducted from August 2018 to December 2018. The model was developed based on the metacognitive experiential learning model (Kolb & Kolb, 2009), competency-based learning management, patient safety principles, and clinical learning (Bott et al., 2011).
Second, evaluating the effectiveness of the developed clinical learning model, which was conducted from January 2019 to February 2019. The evaluation was done quantitatively and qualitatively. In the quantitative strand, a quasi-experimental method using repeated measures design was used. While in the qualitative strand, a qualitative descriptive design was employed.
Participants
Quantitative participants
The population consisted of 96 second-year nursing students. The samples were in the second rotation groups of the 2018 academic year selected using cluster random sampling in wards in which nursing students practice as a sampling unit. The data were collected from 3 out of 12 groups, with eight nursing students in each group. So, a total of 24 nursing students were included in this study.
Qualitative participants
All 24 quantitative participants, two instructors, and one preceptor were included in a qualitative strand.
Instruments
The instruments used in this study were the manual of a clinical learning model, which we developed first before testing to the students. The manual consisted of (1) the principles of the model; (2) the purpose of the model; (3) the DUIR (Doubt, Understanding, Insight, Reflected value) learning process; (5) lesson plans; (6) teaching materials; and (7) learning measurement and evaluation methods. The draft manual was examined by five nursing instructors, two experts in nursing education, and three experts on educational measurements and evaluations, considering the appropriateness of the composition. The results of the validation of the draft manual were the mean score of the DUIR's appropriateness was 4.49 (SD = .50), and the mean score of the lesson plan's appropriateness was 4.53 (SD = .23).
Another instrument was the rubric scoring of patient safety awareness competency, which was developed at the same time as the draft manual by Jutarat Bandansin and colleagues (Bandansin et al., 2020). The rubric scoring was assessed in two components: (1) patient safety management, which consisted of four assessment items, and (2) problem-solving to ensure safety in terms of patient care, which consisted of three assessment items. There were five levels of patient safety awareness, divided by performance quality, from Level 0 to Level 4. Each level of awareness describes behavioral attributes that demonstrate different performance qualities. The total score is 28 points. The score is transformed to percentage and compared with criteria of achievement as follow: Below 60% is level 0 (no awareness); 60-69.99% is level 1 (peripheral awareness); 70-79.99% is level 2, (recognizable awareness); 80-89.99% is level 3 (cognitive awareness); 90-100% is level 4 (valuable awareness).
Data Collection
Quantitative strand
The quantitative data on the effectiveness of the DUIR clinical learning model were collected among 24 nursing students who practiced fundamental nursing in the second semester of the 2018 Academic Year for four weeks.
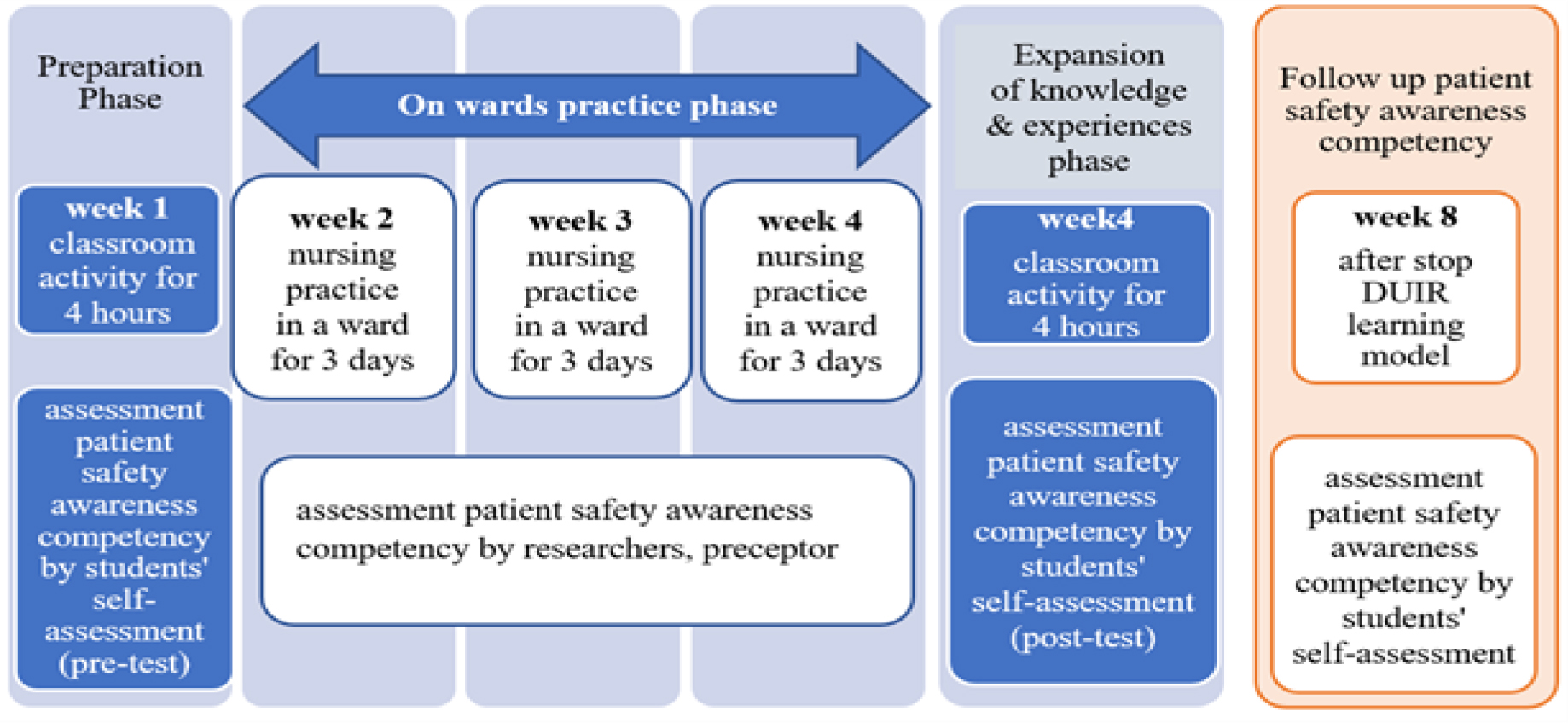
To measure the effectiveness of the DUIR clinical learning model, we employed a quasi-experimental method using repeated measures design, divided into three phases, 1) a preparation phase, 2) a ward practice phase, and 3) an expansion of the knowledge and experience phase. Each phase used the four steps of the DUIR clinical learning process. The performance of patient safety awareness was assessed in week 1 (pre-test), weeks 2, 3, 4 (during learning), week 4 (post-test), and week 8 (after the end of learning), as shown in Figure 1. In addition, the effectiveness of the clinical learning model was measured by researchers, preceptors, and nursing students using scoring rubrics for patient safety awareness competency.
Qualitative strand
We collected qualitative data in 24 students through a reflection. The researchers with the teachers asked the students three questions to write the answer on a blank paper: 1) What was your learning-related patient safety experience? 2) How did you manage the incident? 3) What did you do to protect the harm or prevent the risk if you confronted the new experience? The students described their answers thoroughly. In addition, for two instructors and one preceptor, we conducted in-depth interviews about the clinical learning models’ benefits and obstacles. All interviews were audio-recorded and transcribed verbatim.
Data Analysis
Qualitative data analysis
Quantitative data on the effectiveness of the DUIR clinical learning model were statistically analyzed using SPSS 21.0 to calculate mean score and standard deviation (SD) and to conduct One-way repeated measures ANOVA was as follows: (1) The mean score on nursing students' patient safety awareness competency was assessed by self-assessment after using the learning model; (2) The mean scores on nursing students' patient safety awareness competency, which instructors assessed after using the learning model every week; (3) The comparisons of the variance of the mean score on nursing students' patient safety awareness competency were assessed by instructors each week.
Qualitative data analysis
A content analysis model was used to analyze qualitative data by organizing the qualitative data, open coding, creating categories, and formulating a general description (Elo & Kyngäs, 2008).
Ethical Considerations
This research was approved by the Research Methodology and Ethics of the Institutional Review Board Royal Thai Army Medical Department on 28 August 2018 with Code Q020q/61 and the Ethics Committee of Srinakharinwirot University on 27 August 2018 (Certification number: SWUEC/E-24722561). Furthermore, the informed consent document was obtained from all participants after the researchers explained the study purpose and process. Participating in this study did not affect nursing students’ grades in this subject. A part of this study, the components of patient safety awareness and the rubric scoring of patient safety awareness competency, has been published in a local journal (Bandansin et al., 2020).
Results
Phase 1: DUIR Clinical Learning Model Development
In this phase, the DUIR clinical learning model was established to enhance patient safety awareness among nursing students, which consisted of the principles and the purposes of the clinical learning model, learning process, content, teaching materials, and measurement and evaluation. The four steps of the DUIR process begin with Doubt (D), a step of the risks and harm spotlight. A clinical instructor asks the questions for students to inquire about the risk and the harm related to the patient care process. The second step is Understanding (U), an action to discuss risk and harm prevention in the patient care process. The third step, Insight (I), is a risk and harm checkpoint step before taking procedures or patient care. The fourth step, Reflected value (R), is a step of experience sharing. A clinical instructor asked the reflective questions for students to criticize their risk experiences to improve patient safety performance. It encouraged the students to report their near-miss activity of process care. They had got feedback that made them feel comfortable to report near misses or errors. The DUIR process was a cycle model run in each learning activity (Figure 2).

Phase 2: DUIR Clinical Learning Model Effectiveness
In this phase, the effectiveness of the DUIR clinical learning model was assessed in terms of patient safety awareness behaviors by the students’ self-assessment and the instructors’ assessments in terms of two components: management of the safety patients and solving the problems of insecurity in terms of caring for the patients. The results of the effectiveness of the DUIR clinical learning management model are described in the quantitative and qualitative results.
Quantitative results
The patient safety awareness competency by students’ self-assessment
Before using the DUIR clinical learning model, the overall mean score of the patient safety awareness competency was low (Mean = 9.58, SD ± 3.46). In contrast, at the end of an experimental period (Week 4), the overall mean scores of the patient safety awareness competency were very high (Mean = 23.63, SD ± 3.00), and it remained the same in the follow-up period (Week 8), with a very high level of awareness (Mean = 24.08, SD ± 2.47) (Table 1).
| Measurement Period | Mean score | ± SD | Competency |
|---|---|---|---|
| Before using the model (Week 1) | 9.58 | ± 3.46 | Low Level |
| At the end of the learning process (Week 4) | 23.63 | ± 3.00 | Very High Level |
| Follow-up period (Week 8) | 24.08 | ± 2.47 | Very High Level |
Total score: 28
One-Way Repeated Measures ANOVA was used to compare the mean scores of patient safety awareness competency by the students’ self-assessment, based on three measurements. The results showed that before using the model (Week 1), the end of using the model (Week 4) and the follow-up after stopping the model (Week 8), which at least one pair was significantly different at the .05 level (F = 338.405, df = 1.139, p <.001) (Table 2).
| Source of Variation | SS | df | MS | F | Sig |
|---|---|---|---|---|---|
| Within-Subjects Effects | |||||
| Performance evaluation period (Time) | 3,261.028 | 1.139 | 2862.112 | 338.405* | <.001 |
| Error (time) | 221.639 | 26.206 | 8.458 | ||
The results revealed that the DUIR learning model was more effective in enhancing patient safety awareness competency, with statistical significance at a level of .05. In addition, the mean score at the end of using the model (Week 4) was higher than before using the model (Week 1) (p <.001), and the mean score of the follow-up period after stopping the model (Week 8) was higher than before using the model (Week 1) (p <.001) (Table 3).
| Patient Safety Awareness Competency | Mean Difference | Std. Error | Sig | |
|---|---|---|---|---|
| Before using the model (Week 1) | The end of using the model (Week 4) Follow-up after stop using the model (Week 8) |
-14.05* -14.50* |
.738. .778 |
<.001 <.001 |
| At the end of using the model (Week 4) | Before using the model (Week 1) Follow-up after stop using the model (Week 8) |
14.05* -.45 |
.738 .233 |
<.001 .184 |
| Follow-up after stopping the model (Week 8) | Before using the model (Week 1) The end of using the model (Week 4) |
14.50* .45 |
.778 .233 |
<.001 .184 |
Students’ patient safety awareness competency based on instructors’ assessment after using the learning model every week
The results showed the mean scores on patient safety awareness competency by the assessments of instructors during ward practice. The students’ performances were assessed at the end of ward practice in Week 1, Week 2, and Week 3. The overall mean scores on the patient safety awareness competency of students after using the DUIR learning model were between 80.00-89.99%, which could be interpreted that nursing students had a Level 3 of patient safety awareness (Cognitive Awareness) from a total score, which was at Level 4 (Valuable Awareness) (Table 4).
| Measurement Period | Mean score | ± SD | Competency |
|---|---|---|---|
| Ward Practice in Week 1 | 10.25 (36.61 %) | 1.42 | Low Level |
| Ward Practice in Week 2 | 17.96 (64.14 %) | 2.14 | Intermediate Level |
| Ward Practice in Week 3 | 22.71 (81.10 %) | 1.57 | High Level |
Total score: 28
One-Way Repeated Measures ANOVA results showed that the student performances at the end of ward practice in Week 1, Week 2, and Week 3 differed statistically at a level of .05 (F = 876.270, df = 2, p <.001) (Table 5).
| Source of Variation | SS | df | MS | F | Sig |
|---|---|---|---|---|---|
| Within-Subjects Effects | |||||
| Performance evaluation period (Time) | 1897.528 | 2 | 948.764 | 876.270* | <.001 |
| Error (time) | 49.806 | 46 | 1.083 | ||
*Sphericity Assumed
The instructors assessed the mean scores on patient safety awareness competency. The data showed statistically significant differences (p <.05) in the students’ performance at the end of ward practice in Week 1, Week 2, and Week 3. Therefore, the DUIR learning model effectively enhanced patient safety awareness competency (Table 6).
| Patient Safety Awareness Competency | Mean Difference | Std. Error | Sig | |
|---|---|---|---|---|
| Ward Practice in Week 1 | Ward Practice in Week 2 Ward Practice in Week 3 |
-7.708* -12.458* |
.359 .276 |
<.001 <.001 |
| Ward Practice in Week 2 | Ward Practice in Week 1 Ward Practice in Week 3 |
7.708* -4.750* |
.359 .257 |
<.001 <.001 |
| Ward Practice in Week 3 | Ward Practice in Week 1 Ward Practice in Week 2 |
12.458* 4.750* |
.276 .257 |
<.001 <.001 |
Qualitative results
The qualitative data were analyzed based on the learning reflections and the nursing students’ opinions during ward practice. The results revealed that the nursing activities of the nursing students with patients covered all patient safety awareness competency components. These safety behaviors and outcomes reflected nursing sensitivity outcomes, such as high alert drugs or double-checking, infection control in urinalysis, sputum suction, prevention of injury from physical restraint, prevention of displacement falls, and the recording and reporting of warning signs. In addition, some nursing students focused on their emotions, listening to the patients’ problems and needs, and improving their practices.
Meanwhile, the data analysis from interviews with instructors and preceptors who assisted in supervising the practical training of nursing students revealed that the DUIR clinical learning management model was able to integrate safety principles and concepts with nursing processes for planning and implementation harmoniously. In addition, the safety awareness performance indicated that nursing students would remember procedures and think critically about patients’ clinical risks. The critical success factors for using the learning model were:
The learning model and the contents covered nursing sensitivity outcomes related to patient safety
A questioning technique was used to stimulate safety/risk thinking.
Reflection on learning during the post-conference allowed nursing students to reflect on good performance and errors.
The atmosphere of listening and sharing learning experiences of errors or near-misses, without blaming, and collaboration to inquire about a solution promoted a safety culture.
Discussion
Many patient safety educational interventions proved that patient safety awareness is required for qualified nurses' characters in clinical settings (Tregunno et al., 2014). WHO encouraged healthcare faculties to use the WHO patient safety curriculum guide-multi-professional edition (World Health Organization, 2011) to teach healthcare students, which differ in many ways from the context of preregistration students nurses, the curriculum in each discipline, the policy of clinical workplace, and previous clinical experiences of the clinical instructors. In fact, in the context of this study, there is still a gap in the nursing curriculum in which patient safety content is limited or unclear to be integrated into practice, thus unable to connect to the real-world situation (Mansour et al., 2015).
The DUIR clinical learning model was developed from a competency-based concept and a metacognitive experiential learning model to effectively enhance student patient safety awareness competency. This clinical learning model promotes learning outcomes, which demonstrate nursing students' patient safety awareness competency in two components: patient safety management (risk detection, safety nursing practice, awareness, and compassionate response to patient needs, communication for effective nursing care) and problem-solving to provide safe care (exchanging experiences learned about patient safety, improving nursing plans to prevent patient risks, and participating in solving safety problems into patient care). These components, however, are in accordance with the patient safety competency framework of The Quality & Safety Education for Nursing (QSEN), which states that patient safety competency is based on patient-centered care that focuses on the risks that affect the body and takes into account the emotions of the patient and their relatives to promote compassionate care for the patient based on respect for the patient's values, beliefs, values or needs.
Additionally, instilling a safety culture among nursing students as part of the nursing care team can protect their patients' safety and promote efficient communication with patients, the nursing team, and the multidisciplinary (Cresswell et al., 2013; DeBourgh, 2012). The learning model is also consistent with the components of patient safety performance measurement of registered nurses in Thailand regarding individual factors affecting patient safety, emphasizing examination of readiness or limitation of knowledge and skills in working. Furthermore, there are good attitudes of following the patient safety principles and practices protocol, including participating in safety cultures, such as communicating with the nursing team about warning signs of the patients, reporting errors or near-miss incidence (Panthulawan et al., 2016). Hence, the learning outcomes are determined to relate to nursing sensitivity outcomes (DeBourgh, 2012; Gravina, 2017; Lee et al., 2014), and Thailand Safety Goals (SIMPLE - Safe surgery, Infectious control, Medication error, Process care, Line and tube safety, Emergency response) (Limpanyalert, 2018; Panthulawan et al., 2016).
The influence of the clinical learning model or DUIR model on learners’ patient safety awareness competency in this study could be described from its learning process. For example, in Step 1 (Doubt) and Step 2 (Understanding focused on the thinking process by questioning related to risk or patient safety during clinical practice), the lessons learned from past mistakes influenced learners to think about how and why it happened and the chance of it happening in the future (Taitz et al., 2010; World Health Organization, 2017). At this point, nursing care plans and actions can be influenced by the ability to understand the risks or opportunities for the hazard. That ability predicts the outcomes if the nursing plans and standard practice guidelines are not followed. In addition, human factor errors can be reduced or eliminated by accepting and believing in standard operating procedures and analyzing various errors that have occurred in the past (Cresswell et al., 2013; Steven et al., 2019). In Step 3 (Insight, access to safety), compliance with standard practice, essential skills in performing tasks, and linking patient safety issues with ethical standards and professional ethics were emphasized. This will help nurture learners to realize the importance of the problem and its impact on patients and themselves. Meanwhile, in Step 4 (reflecting the value), the thinking process was the main focus by reflecting on work experiences, questioning and linking them to patient safety that will help learners realize the importance of actions to prevent or reduce the risk of danger with patients (Steven et al., 2019). Therefore, this clinical learning model affected the mean scores of the patient safety awareness competency among students, with a high level.
The patient safety awareness performance scores were consistent with the qualitative data from students' learning reflections and the instructors' experience sharing. They agreed with memorizing procedures and practicing each method until fluency skills are not enough to enrich safety performance. Students must reflect on what they have learned from errors or near-missed experiences and describe how to prevent that from happening again. These findings, however, were consistent with the study of patient safety competency among Bachelor's degree nursing students using an integrative literature review (Tella et al., 2014), and found that the strategies for learning management promoted patient safety competence, such as creating a conducive environment for learning, practical learning and reflection practice on patient safety in various situations (Tella et al., 2014).
In terms of critical reflection, in the DUIR model, the teachers acted as a coach or facilitator in learning by stimulating the thinking of learners by using questions to assess their understanding of knowledge or practice. After performing procedures with patients, reflective questions also allow the learners to explore and review their thoughts and then analyze them. According to Stoddard and O’Dell (2016), practice can change the attitudes and behaviors of learners. In addition, metacognition is used to develop ethics, and learners use situations to stimulate thinking and then express behavior or opinions by writing a description of their feelings or answering interview questions that reflect their beliefs, values, and ethical behavior (Seibert, 2014). However, this strategy is consistent with the study using questioning to reflect the feelings of emergency nurses, especially communication in their work, which affected emergency nurses in dealing with various patient safety situations (Pangh et al., 2019). So, it can be said that attitude and non-technical skills such as communication, critical thinking, problem-solving, empathy, and collaborative skills are essential to support patient safety performance.
Last, it is noteworthy that the DUIR learning process encouraged nursing students to reflect on mistakes or near misses, sharing problem-solving experiences, emotions, and feelings related to problems, risks, or hazards to patients. As a result, learners immersed themselves in problem processes, learning to transform their behaviors for quality and patient safety nursing outcomes (Colet et al., 2015; Steven et al., 2019). Therefore, the learning process stimulated a thought to criticize experience by questioning patient safety improvement.
Limitations
The quantitative study design that did not have a control group might affect the effectiveness of the DUIR learning model, which could be considered a limitation. However, this study used the repeated measures design to control factors that cause variability between subjects. Moreover, this design could track the effect over time and better measure the same subject multiple times rather than different subjects at one point in time.
Implications for Nursing Education
This study could be served as input for nurse educators to use the DUIR learning model in their teaching-learning process. The DUIR learning model is operated in both the classroom and clinics by the teachers and preceptors, providing nursing students time to think and wait for an answer in a low-pressure environment. Additionally, the teachers listen and observe the body language when the students answer the question on how they feel about risk or harm with patient outcomes. The teachers should not be too quick to judge but should encourage nursing students to reflect on their learning performance. So, the students will be able to criticize their practice to achieve quality and safe care outcomes.
Conclusion
The developed DUIR clinical learning model has four steps: (1) Doubt (D); (2) Understanding (U); (3) Insight (I); and (4) Reflected Value (R). This learning model used metacognitive thinking through experiential learning by using questioning strategies as a tool for patient safety learning and assists the learners to doubt and ask questions about their experiences related to the safety of nursing activities with patients. Therefore, the model can be considered effective. Furthermore, it can be applied in both classrooms and clinics, which the teachers and preceptors act as facilitators lead students to criticize their practice without judgments and encourage students to report the errors or near-misses in order to enhance patient safety awareness among nursing students with confidence and to be able to transform their practice focusing on the quality and safe patient care outcomes.