









Background
The current scenario of chronic conditions keeps health care providers in a dilemma. As the elderly population increases around the globe, chronic conditions remain steadily become part of the challenges. Chronic disease, especially diabetes mellitus, keeps health care providers in check. The annual figures were shown an increasing trend worldwide, including in low and middle-income countries (International Diabetes Federation, 2013; World Health Organization, 2016). In Malaysia, a similar increasing trend was reported in diabetic conditions (Feisul & Azmi, 2013).
Health promotion is one of the essential aspects of health care delivery. However, health promotion should be more reliant on addressing chronic conditions (Kumar & Preetha, 2012; Ydirin, 2021). In the current era of the industrial revolution, known as IR 4.0, the booming technological advances greatly affect individuals daily. Indirectly, health care transformation did occur, affected by global changes of the new IR 4.0 era, especially in addressing care of chronic conditions. eHealth tools such as telemedicine, mobile health application (mHealth), or teleconference are among the options available in the delivery of care; ehealth tool is an electronic technology used in the delivery of health care information and communication (World Health Organization, 2022).
Self-management is another important aspect closely related to health promotion when managing chronic conditions, especially for patients with diabetes. Positive outcomes were noted in behavior modification when managing chronic diseases, especially in diabetes management (Baumann et al., 2015; Debussche et al., 2018; Kurniawan, 2011; Pamungkas, 2015; Primanda et al., 2011; Ramadas et al., 2018; Thojampa & Acob, 2020). Thus, self-management should be emphasized among the patient, especially in a primary care setting.
With the advancement of technology, self-management should be embedded together so that health care delivery can be performed innovatively. According to the literature review conducted, it is found that a technology-friendly program would be very helpful in managing diabetes foot care (Firdaus & Jittanoon, 2021). For instance, in managing diabetes conditions, there were many technology-based interventions available such as a multisite telehealth program (Ciemins et al., 2018), the Norwegian study of RENEWING HEALTH (Holmen et al., 2016), an SMS application program (Naghibi et al., 2015), a telemedicine program (Kolltveit et al., 2017), a mobile phone diabetes project for Chicago Plan (CareSmart) (Nundy et al., 2014), diabetes guidelines adherence via SMS (Hashmi & Khan, 2018) and the Mobile Diabetes Intervention Study, a web-based personalized program (Quinn et al., 2009).
These technological-based interventions have shown positive findings as follows; 1) physiological outcomes such as blood profiles (Nundy et al., 2014; Quinn et al., 2009) and body weight (Ciemins et al., 2018; Holmen et al., 2016), 2) engagement in physical activity (Ciemins et al., 2018; Holmen et al., 2016), 3) dietary management (Ciemins et al., 2018), and 4) adherence to treatment or diabetes guidelines (Hashmi & Khan, 2018; Naghibi et al., 2015; Nundy et al., 2014).
However, most existing technology-based intervention programs focus on general diabetes care rather than foot care. The foot care component was included as only a minor component in the programs. There is little evidence of any mobile health study focusing on diabetes foot care specifically. With the promising possible outcomes, a mobile health application program was chosen to be an alternative technology-based intervention program employed in the study. Additionally, virtual care novelty was introduced by using technology-based intervention in managing diabetes foot care. This approach would be greatly beneficial to health care providers since virtual care can be delivered to the patient. Indirectly, issues of staff shortage, less specifically trained staff, and long waiting times at the clinic can be addressed (Abazari et al., 2012; Hussein et al., 2015).
A careful process should be conducted to develop a new mobile health application imbued with self-management concepts. Thus, this paper intends to elaborate on the process of developing, validating, and pre-testing the Diabetic Care Self-Management Mobile Health Application (Diabetic Care) developed by the researchers.
Methods
There are two phases involved in the process of developing, validating, and pre-testing the Diabetic Care app. In the first phase, the Diabetic Care app was developed and tested for content validity, while in the second phase, the mobile app was pre-testing among patients with diabetes.
First Phase: Developing and Examining the Content validity of the App
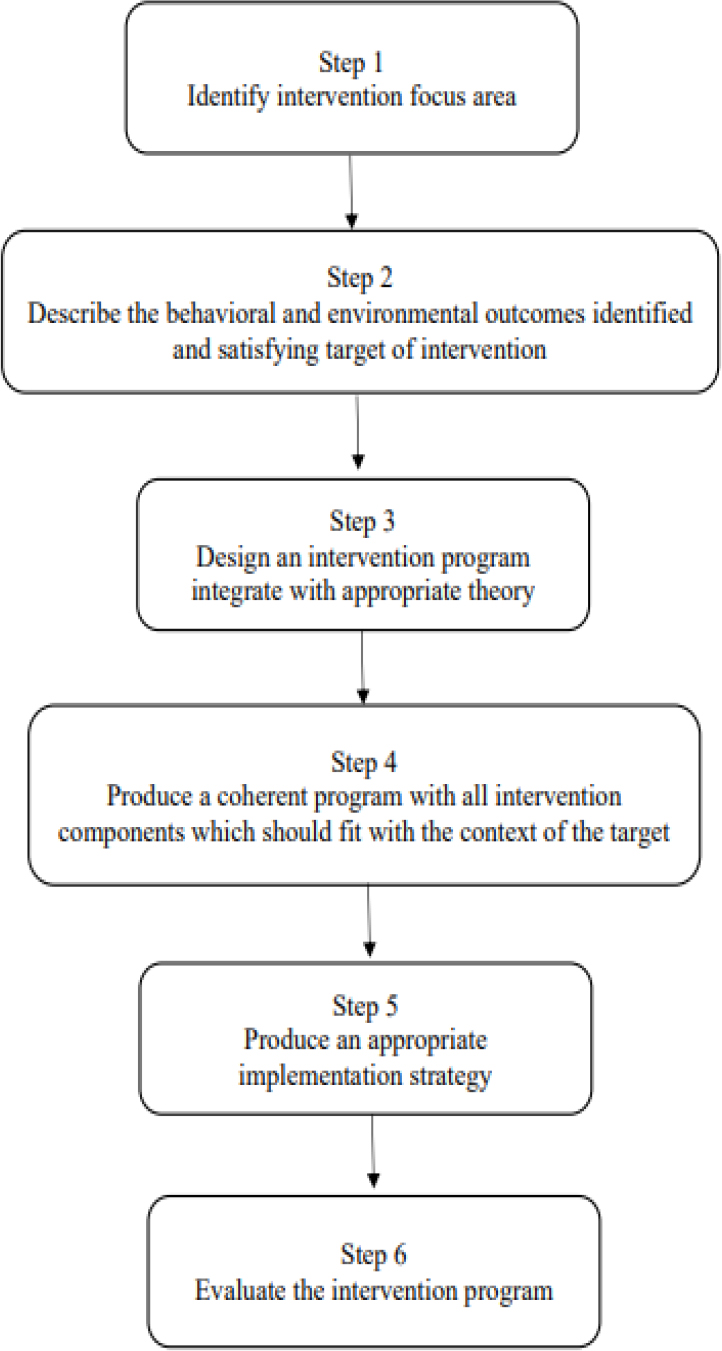
In the first phase, the process of developing mobile health app was guided according to the Intervention Mapping (IM) Framework by Fernandez et al. (2019). The IM was used to ensure the mobile health app developed was designed and rendered empirical evidence with sound theories. There are six steps in IM when developing an interventional program for health promotion (Eldredge et al., 2016). The first step is identifying the intervention focus area by thoroughly understanding the health-related problem, the population at risk, the determinants of these behavioral and environmental conditions, and assessing available resources. Next, the issues concerning uncontrolled diabetes mellitus in Malaysia were explored. The results showed that diabetic foot complications and uncontrolled blood sugar were listed among the most typical challenges in uncontrolled diabetes mellitus in Malaysia (Mazlina et al., 2011; Syed Soffian et al., 2019).
In the second step of IM, the description of behavioral and environmental outcomes was identified, specifying the target of the intervention. In this study, the behavioral determinants identified were foot care behavior and dietary behavior, while the environmental determinants were related to self-management via assisted mobile health applications. In addition, foot care and dietary behavior are closely related to foot conditions and fasting blood sugar control. Therefore, this study included these two secondary outcomes as assessing variables. The main objective of this program is to assist with self-management via mobile health applications on foot care behavior and dietary behavior among uncontrolled diabetes mellitus.
In the third step of IM, a theory-based intervention should be selected to guide the design of the program. The Individual and Family Self-Management Theory by Ryan and Sawin (2009) was chosen to guide the development of the Diabetic Care Self-Management Mobile Health Application. The theory was chosen after an analysis was conducted to select the most appropriate theory that can be employed in this study.
In this theory, four important dimensions need to be understood. The dimensions were: a contextual factor, the process of self-management, and two separate outcomes: distal and proximal. In the contextual factor dimension, there was an individual factor, a condition-specific factor, and the physical and social environment. Considering all of these factors, mobile health apps were developed accordingly. For instance, individual factors were age, gender, level of education, and ethnicity. The app used the simplest language possible and was produced in bilingual (English and Malay) by considering various potential ages, genders, levels of education, and ethnicities of the eventual user. With the condition-specific factors, the app was designed based on the need to emphasize the self-management of their diabetic condition. Thus, all information provided in the apps was specifically related to managing the diabetic condition. With the physical and social environment factors, the app was developed by addressing the issues of remote access to care for the user. By installing this app, the user can use it in any place and at any time.
For the process of self-management dimension, the factors of knowledge and belief, self-regulation skills and abilities, and social facilitation were considered during the app development. Various methods of knowledge sharing in the app were employed, such as videos of foot care activities, combined with simple text explanations and a diagram to emphasize knowledge of diabetic management. In addition, the video was also functioning as a user’s referral for developing self-regulation skills in diabetic self-care. The use of various audiovisuals can positively influence behavior modification among patients with diabetes (Rahaman et al., 2018).
Lastly, in the outcomes dimension, two different outcomes were identified by Ryan and Sawin (2009), namely, distal and proximal. The distal outcome is related to behavioral modification, while the proximal outcome is related to physiological body changes. Considering both distal and proximal outcomes, the app was developed to promote better health behavior which can be assessed through behavior modification (distal outcomes) by improving foot care behavior and dietary behavior. Inversely, foot condition and fasting blood glucose levels were physiological changes (proximal outcomes) that may be observed in the user’s body. Hence, considering the concept of self-management and mobile health application together with the identified outcomes, a mobile health app was developed and named ‘Diabetic Care Self-Management Mobile Health Application (Diabetic Care).’ The Diabetic Care app was designed to focus on promoting foot care behavior and dietary behavior.
The fourth step of IM is developing a coherent program by combining all intervention components that should fit the target context. The intervention components in this study are the use of the developed mobile app (Diabetic Care app) together with the conventional method that existed in the current setting. The conventional approach is to provide health education while patients are in the clinic for follow-up appointments.
The next step in the IM is that an appropriate implementation strategy should be developed to facilitate the usefulness and sustainability of the program. Hence in this study, a protocol for the intervention was developed to facilitate the intervention. Thus, a clear direction for the intervention implemented was able to be maintained and ensured that it was standardized towards the end of the intervention period.
Lastly, to assess the effectiveness of the program, an evaluation should be carried out as the last step in IM. A pilot study was conducted so that any discrepancies or shortcomings could be detected. Thus, appropriate action can be planned to overcome the problems or challenges identified in the earlier process. The pilot study was conducted as recommended in IM. The summary of IM can be seen in Figure 1.
When the application was ready, a content validity inspection was conducted. Content validity of the apps was inspected by employing Kassam-Adams et al. (2015)’s guidance specifically for assessing the eHealth tool. There were three important components: relevance, likely effectiveness, and appropriateness. In determining the relevance component, the relevance of a theory chosen with the developed app was checked as to whether each specific intervention activity identified in the application is appropriate for the intended intervention target. The effectiveness component assessed the effectiveness of the apps’ components and their likelihood to influence the behavior modification of the intended intervention target.
While the appropriateness component was investigated for the Malaysian population according to the language used, nature of the activities, comprehensible instructions provided, and cultural appropriateness. A Likert Scale of 1 (not good) to 4 (most suitable or relevant) was employed in the content validity survey for each domain. A score of 3 to 4 is considered good, while a score of 1 to 2 indicates revision required for the mobile application, then rerun for another cycle of content validity checking. For each score, sections scored with 3 to 4 were converted into relevance (1 mark), while a score of 1 to 2 was converted into irrelevant (0 mark). Finally, a total score was calculated by averaging the total mark from each expert divided by the universal agreement. The content validity was inspected by a group of experts. They were a diabetes nurse educator, a dietitian, and a medical officer in charge of non-communicable diseases at the district level. The team of experts is the people who are actively involved in their day-to-day managing patients with diabetes mellitus conditions.
Second Phase: Pre-testing the Mobile App
In this phase, the app was tried out among patients with diabetes in the primary care setting. Ten patients were invited conveniently to pre-testing the app to be used as an intervention tool. The invitation was sent individually to all patients through WhatsApp.
Ethical Consideration
Ethical approvals were sought from the Social and Behavioral Sciences Institutional Review Board, Faculty of Nursing, Prince of Songkla University, Hat Yai, Thailand (Certificate No: PSU IRB 2019 – NSt 017) and Medical Research Ethics Committee, Ministry of Health Malaysia (NMRR-19-3168-51578(IIR)).
Results
Phase 1: Development of the App
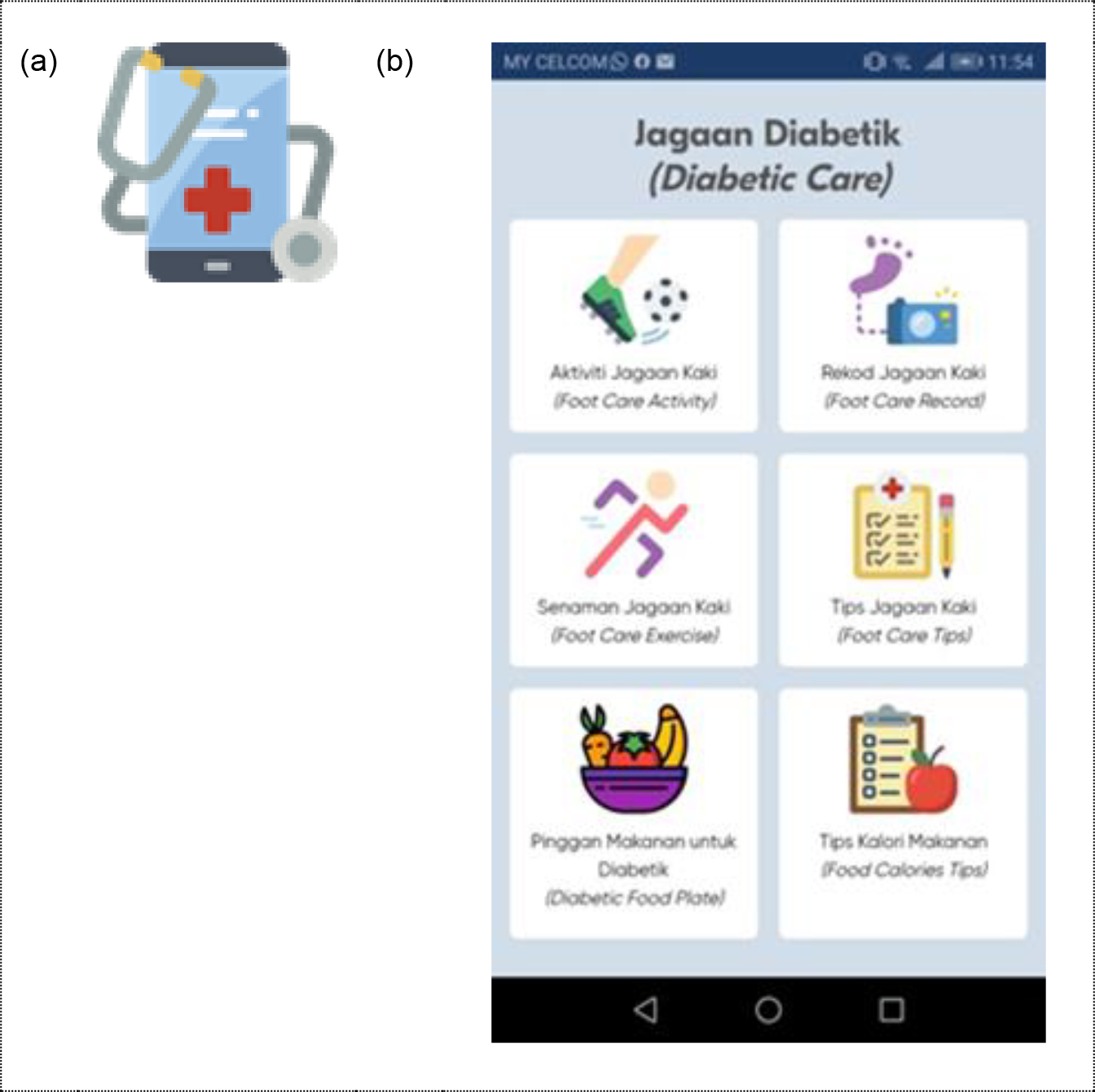
Six components of the Diabetic Care Self-Management Mobile Health Application were represented by six different icon buttons. They were 1) diabetic foot care activities, 2) foot care exercise, 3) foot care tips, 4) foot care records, 5) diabetic food plate guidelines, and 6) food calorie tips. All the icons were made by Freepik.com, smalllikeart, fjsstudio, and Nikita Golubev from www.flaticon.com, which are free to use. In diabetic foot care activities, there were four sub-components: foot washing, foot inspection, trimming nails, and applying lotion. All of these were linked to a separate video provided by the researcher. This video was used for reference by the app user. Similarly, for the foot care exercise, there were five sub-components labeled Exercise 1 through 5 with five different foot care exercises. When the user clicked on the label of the exercise, the user was provided with a video of the foot care exercise in each sub-component. For foot care tips, the user was given tips for best-practice foot care.
The foot care record was functioning as a diary app. There was a table under this icon consisting of foot washing, foot inspection, trimming nails, and applying lotion. The table was synced with the date, and the user needed to click on the table whenever they performed the foot care activities listed. The foot care record was connected to a cloud database. The information the user put into the foot care record was accessible by the researcher through a cloud database.
In the diabetic foot care food plate sub-component, the user was provided with a diagram of the food plate suggested for patients with diabetes. This functioned as a reference source for the user. Lastly, for food calorie tips, the user was given a list of basic food usually taken according to a Malaysian context, with the total calories as advised for their daily life. All of the content in the mobile health application was designed according to the clinical practice guidelines such as Diabetes Education Manual 2016 (The Malaysian Diabetes Educator Society, 2016), Clinical Practice Guidelines Management of Type 2 Diabetes Mellitus (5th Edition) (Ministry of Health Malaysia, 2015), Clinical Practice Guidelines Management of Diabetic Foot (2nd Edition) (Ministry of Health Malaysia, 2018a), and information extracted from Ministry of Health Malaysia’s website (Ministry of Health Malaysia, 2016, 2018b; Nor, 2013). The summary of Diabetic Care is shown in Figure 2.
Phase 2: Content Validity and Pre-testing of the App
There are 16 sections identified for the assessment of content validity on the Diabetic Care Self-Management Mobile Health Application. The sections were: 1) Diabetic Care main menus; 2) Foot Care Activity menus; 3) Washing Feet; 4) Trimming Nails; 5) Foot Inspection; 6) Applying Lotion; 7) Foot Care Exercise menus; 8) Exercise 1; 9), Exercise 2; 10), Exercise 3; 11) Exercise 4; 12) Exercise 5; 13) Foot Care Record menus; 14) Foot Care Tips; 15) Diabetic Food Plate menus, and 16) Food Calorie Tips menus. The experts were required to rate sixteen sections according to the components of relevance, likely effectiveness, and appropriateness.
In the content validity assessment, all 16 sections were scored between 3 to 4 by all three health experts in all identified components (relevance, likely effectiveness, and appropriateness). The CVI score for the mobile health app was shown as 1.00 for all sections. Likewise, a good general CVI score of 1.00 was noted for the Diabetic Care Self-Management Mobile Health Application (See Table 1).
| Items | Relevance | Likely Effectiveness | Appropriateness | ||||||||||
|---|---|---|---|---|---|---|---|---|---|---|---|---|---|
| E1 | E2 | E3 | I-CVI | E1 | E2 | E3 | I-CVI | E1 | E2 | E3 | I-CVI | ||
| Section 1 | 4 | 4 | 4 | 1.00 | 4 | 4 | 4 | 1.00 | 4 | 4 | 4 | 1.00 | |
| Section 2 | 4 | 4 | 4 | 1.00 | 4 | 4 | 4 | 1.00 | 4 | 4 | 4 | 1.00 | |
| Section 3 | 4 | 4 | 4 | 1.00 | 4 | 4 | 3 | 1.00 | 4 | 4 | 3 | 1.00 | |
| Section 3 | 4 | 4 | 4 | 1.00 | 4 | 4 | 3 | 1.00 | 4 | 4 | 3 | 1.00 | |
| Section 4 | 4 | 4 | 4 | 1.00 | 4 | 4 | 4 | 1.00 | 4 | 4 | 4 | 1.00 | |
| Section 5 | 4 | 4 | 4 | 1.00 | 4 | 4 | 4 | 1.00 | 4 | 4 | 4 | 1.00 | |
| Section 6 | 4 | 4 | 3 | 1.00 | 4 | 4 | 3 | 1.00 | 4 | 4 | 3 | 1.00 | |
| Section 7 | 4 | 4 | 4 | 1.00 | 4 | 4 | 4 | 1.00 | 4 | 4 | 4 | 1.00 | |
| Section 8 | 4 | 4 | 4 | 1.00 | 4 | 4 | 4 | 1.00 | 4 | 4 | 4 | 1.00 | |
| Section 9 | 4 | 4 | 4 | 1.00 | 4 | 4 | 4 | 1.00 | 4 | 4 | 4 | 1.00 | |
| Section 10 | 4 | 4 | 4 | 1.00 | 4 | 4 | 4 | 1.00 | 4 | 4 | 4 | 1.00 | |
| Section 11 | 4 | 4 | 4 | 1.00 | 4 | 4 | 4 | 1.00 | 4 | 4 | 4 | 1.00 | |
| Section 12 | 4 | 4 | 4 | 1.00 | 4 | 4 | 4 | 1.00 | 4 | 4 | 4 | 1.00 | |
| Section 13 | 4 | 4 | 4 | 1.00 | 4 | 4 | 3 | 1.00 | 4 | 4 | 3 | 1.00 | |
| Section 14 | 4 | 4 | 3 | 1.00 | 3 | 4 | 3 | 1.00 | 3 | 4 | 3 | 1.00 | |
| Section 15 | 4 | 4 | 4 | 1.00 | 4 | 4 | 4 | 1.00 | 4 | 4 | 4 | 1.00 | |
| Section 16 | 4 | 3 | 3 | 1.00 | 3 | 3 | 3 | 1.00 | 3 | 3 | 3 | 1.00 | |
| S-CVI | 1.00 | 1.00 | 1.00 | ||||||||||
Notes. E = Expert, I-CVI = Item content validity index, S-CVI = General content validity index for the app
A pilot test was conducted to examine the Diabetic Care Self-Management Mobile Health Application among ten conveniently chosen patients with diabetes at a governmental primary care-run clinic. The test was conducted in the middle of February 2020. The app is plausible to be used as an intervention tool. The patients were able to download and use the app. However, two challenges were identified during the pilot testing of the mobile app. Out of ten patients who were trying the app, three patients encountered difficulties during the download process of the app. The second challenge was related to the function of the Foot Care Record.
Discussion
In the validity assessment of the Diabetic Care Self-Management Mobile Health Application, all of the experts agreed that the mobile application was relevant, appropriate, and more likely to be effective in behavior modification. With three experts in a team, a CVI score of 1.00 should be acquired for the tool to be classified as good (Polit et al., 2007; Yusoff, 2019). The CVI score of 1.00 showed that the app was good for use. However, two obstacles were found during the test out of the application among ten patients. Firstly, the installation of the Diabetic Care Self-Management Mobile Health Application was invited through WhatsApp. However, three patients encountered problems during the process of sharing. Thus, an alternative method was explored for instances by using ShareIt, Bluetooth, and email applications. Out of the three ways explored, the ShareIt application was shown as a promising alternative in installing Diabetic Care Self-Management Mobile Health Application in a shorter duration, while Bluetooth and email took a long time.
Secondly, the problem is related to the function of the foot care record in the Diabetic Care Self-Management Mobile Health Application. In this part, the user needs to record foot care activities throughout the week. However, when the foot care record function was fully utilized within one week, the apps needed to be cleared manually by the researcher through a cloud database. Thus, the researcher needed to keep this updated every week so that the foot care record is available to be used. In addition, the intervention protocol was provided with a schedule for each patient to monitor daily. Each week the patient was reviewed individually in regards to their learning contract. Hence, the day of reviewing the learning contracts was the same day indicated for the researcher to clear the foot care record section.
Even though two obstacles were detected in translating the Diabetic Care App during the pilot testing, the benefit of the Diabetic Care App outweighs the obstacles. The content of Diabetic Care Apps was developed according to the approved clinical practice guidelines (CPG) by the Ministry of Health Malaysia. The content was extracted from CPG Management of Diabetes Mellitus, 5th Edition (Ministry of Health Malaysia, 2015), CPG Management of Diabetic Foot, 2nd Edition (Ministry of Health Malaysia, 2018a), Diabetes Education Manual 2016 (The Malaysian Diabetes Educator Society, 2016), Diabetic Meal Plan (Nor, 2013) and official government own website; www.infosihat.gov.my. Hence, all the verified contents and information shared with the patient with diabetes is similar to the practices that existed in the Ministry of Health Malaysia setting and firsthand resources.
Besides, the use of various visual aids in presenting information for the patient with diabetes is helpful for the information to be well delivered. The use of video and diagrams has shown positive findings in increasing knowledge among patients during the health education process (Calderón et al., 2014; Gerber et al., 2005; Tuong et al., 2014). Integration of various visual aids such as diagrams, videos, and bullet list information is employed in the Diabetic Care App. A diagram is used to deliver the guidance for appropriate dietary portion guidance, a video for foot care exercises and foot care activities, and bullet list information for foot care tips and food calorie tips.
Another good thing about Diabetic Care App, the app developed is accessible at any place or anytime. The patients may refer to the app whenever at their own pace. Hence, dynamic promotion of health education can be emphasized for better foot care and dietary behavior according to the patient preference. Personal space with a homely, welcoming atmosphere and a supportive environment may affect patient engagement in rehabilitation activities (Douglas & Douglas, 2004). Indirectly this important feature may reflect that virtual care is possible to be done in the primary care setting. It will help the nurses deliver health care promotion better and provide comprehensive patient coverage without time and space limitations.
Moreover, by implementing the app, the number of physical staff required to cater to the patient may reduce. Therefore, the issue of the shortage of qualified trained staff (diabetes nurse educators) is addressed. Additionally, the qualified skilled staff (diabetes nurse educators) charged for the care delivery via app might be as well-appointed as the care delivery person. Therefore, indirectly, better care quality can be provided by the trained staff (diabetes nurse educators) even though their numbers might as well be limited in the setting.
However, a limitation was identified in Diabetic Care App. The app is only suitable for android phones and cannot be used on other types of phones (IOS etc.). Since the app is a pilot project and requires good financial support, the app was made available with the commonest types of phones among Malaysians. Android phone is the most familiar type of phone accessible by the general Malaysian population compared to the IOS phone. It is recommended that the app be the extent to IOS in the future. Therefore, it will also benefit those with an IOS phone.
Conclusion
In conclusion, the Diabetes Care App was given a good CVI score after being assessed by a team of experts. The app was found to be relevant, likely to be effective, and appropriate to be used in the actual data collection. Even though there were two problems noted during the translation of the Diabetes Care Self-Management Mobile Health Application among patients with diabetes at the initial stage, a possible solution was explored immediately to address the issues. Thus, the problems were addressed properly with a solution so that the translation of the app among patients with diabetes was not disturbed. Further research is recommended to be conducted to examine the effectiveness of the mobile app in facilitating behavior modification (foot care and dietary behavior).