









Background
Diabetes mellitus is a chronic condition that may affect an individual living in a long-term condition. The prevalence of diabetes mellitus has increased globally (International Diabetes Federation, 2013; World Health Organization (WHO), 2016), including in Malaysia (Ministry of Health Malaysia, 2014). Diabetes condition was categorized as uncontrolled if the HbA1c reading was > 6.5% (Handelsman et al., 2015; Ministry of Health Malaysia, 2015; The International Expert Committee, 2009). In Malaysia, the prevalence of uncontrolled diabetes showed a worrisome figure (Feisul & Azmi, 2013). Uncontrolled diabetes mellitus will lead to unwanted complications, such as neuropathy, nephropathy, foot complications, and many more.
A diabetic foot ulcer is one of the most common foot complications that may develop. The greatest concern among diabetic patients is susceptibility to a diabetic foot ulcer (Green-Morris, 2014). Among Malaysians, diabetic neuropathy and foot complications contributed 63.7% and 47.8%, respectively, in terms of diabetes mellitus complications related to feet, based on a DiabCare study in 2008 (Mafauzy et al., 2011). Untreated diabetic foot ulcers may lead to amputation, which might as well affect the patient’s quality of life (Fejfarová et al., 2014).
In Malaysia, although there are programs aimed at foot care (Mafauzy et al., 2016), there are still many cases of diabetic foot ulcer incidence (Mafauzy et al., 2011). There are six factors identified that may contribute to poor foot care practices among diabetes patients. Lack of or average knowledge (Abu-elenin et al., 2018; Coffey et al., 2019; Lucio, 2013), poor communication between patients and healthcare providers (Abu-elenin et al., 2018), patient’s self-perception that performing foot care is not essential (Coffey et al., 2019), disregard foot care recommendation provided (Coffey et al., 2019), lack of visible symptoms and gradual onset of diabetic foot ulcers (Coffey et al., 2019) and deterioration of physical health and cognitive limitations (Coffey et al., 2019).
Many diabetic foot care education programs have been carried out to counter the problem of diabetic foot ulcer incidence globally. They are structured teaching and examining program (Ahmad Sharoni et al., 2018; Lavery et al., 2007), intensive monitoring and one-to-one approach (Saurabh et al., 2014; Viswanathan et al., 2005), and group education with a system to monitor adherence, such as the Prophylactic Foot Care Program (Calle-Pascual et al., 2001), and The Lousiana State University Health Sciences Center Diabetes Foot Program (Patout Jr et al., 2000), use of advanced technologies such as infrared thermometers (Lavery et al., 2007) and integrating peer-led empowerment into diabetic education (Baumann et al., 2015).
All of these studies show positive findings regarding foot care behavior (Ahmad Sharoni et al., 2018; Calle-Pascual et al., 2001; Fan et al., 2013), self-efficacy (Ahmad Sharoni et al., 2018; Fan et al., 2013) and empowerment of diabetes self-management (Debussche et al., 2018; Patout Jr et al., 2000). Further literature review showed many studies incorporate mobile health applications related to diabetes care, but they focus on general care. The following existing mobile health programs were identified: a multisite telehealth program (Ciemins et al., 2018), the Norwegian study RENEWING HEALTH (Holmen et al., 2016), an SMS application (Naghibi et al., 2015), a telemedicine program (Kolltveit et al., 2017), a mobile phone diabetes project for Chicago Plan (CareSmart) (Nundy et al., 2014), diabetes guidelines adherence via SMS (Hashmi & Khan, 2018), and the Mobile Diabetes Intervention Study (Quinn et al., 2009).
These mobile health programs showed positive findings regarding physiological outcomes such as blood profiles (Nundy et al., 2014; Quinn et al., 2009) and body weight (Ciemins et al., 2018; Holmen et al., 2016), engagement in physical activity (Ciemins et al., 2018; Holmen et al., 2016), dietary management (Ciemins et al., 2018) and adherence to treatment or diabetes guidelines (Hashmi & Khan, 2018; Naghibi et al., 2015; Nundy et al., 2014). They show that mobile health is a promising alternative in the digital era. However, in all these mobile health programs, foot care was included as only a minor component, and there is little evidence of any mobile health study focusing on diabetic foot care specifically. Therefore, an exploration of the use of a mobile health application, together with the self-management concept, was employed in this study.
Managing foot care requires a holistic approach, including glucose management, dietary management, and lifestyle management, which contributes majorly to managing diabetes conditions generally. Hence, dietary behavior, together with fasting blood glucose and foot conditions, were included in this study apart from foot care behavior.
The Individual and Family Self-Management Theory (IFSMT) by Ryan and Sawin (2009) was used as theoretical guidance in this study. IFSMT comprises three dimensions: contextual factors, process factors, and outcomes (Ryan & Sawin, 2009). Identifying contextual factors (personal characteristics, socio-economic status) helps in the processing of self-management, measured in the outcomes identified (foot care behavior, dietary behavior, fasting blood glucose, and foot conditions). All dimensions of the theory were addressed in this study appropriately. Hence, in this study, the objective was to investigate the effect of the Diabetic Care App on foot care behavior, dietary behavior, fasting blood glucose, and foot conditions among patients with uncontrolled diabetes in Malaysia.
Methods
Study Design
This single randomized controlled trial with two groups of the pretest-posttest study was conducted at a governmental-run primary clinic in Northern Malaysia. There were two outcomes tabulated in this study, known as primary and secondary outcomes. Primary outcomes were related to behavioral modifications such as foot care and dietary behavior while fasting blood glucose and foot condition were secondary outcomes.
Samples/Participants
The patient was recruited according to the following criteria: last two readings of A1c more than 6.5% (Ministry of Health Malaysia, 2015), has at least Stage 1 or above risk of foot ulcer development, aged 18 to 65 years old, has no history of diabetic foot ulcer, able to perform self-care independently, able to use mobile application program, owns an android phone, has no vision or hearing problems that may interfere with process of data collection or the intervention carried out and able to communicate in either English or Bahasa Malaysia (a native and official language of the country). Minimization software version 2.01 was employed in determining the patient’s group. A total of 68 patients were enrolled in the initial program, while 58 were completed at the end of the five-week program. The assessment was carried out in Week 1 and Week 5.
To calculate a reasonable sample size, the effect size can be estimated by similar work published by others (Sullivan & Feinn, 2012). The sample size was calculated based on the effect size identified from each of the dependent variables, such as 0.86 for foot care behavior (Biçer & Enç, 2016), 0.88 for dietary behavior (Ramadas et al., 2018) and 0.81 for fasting blood glucose (Pamungkas, 2015). According to Cohen (1988), the value of effect size is categorized as small (0.2), medium (0.5) and large (0.8). Considering the influence of population variability, differences in demographic background, and accuracy of the instrument employed, a medium to large effect size was chosen, which is 0.7 (less than the effect size obtained from the previous literature calculated) (Sullivan & Feinn, 2012). Assuming a paired t-test with an alpha value of 0.5 and power of 80%, with an effect size of 0.7, the sample size required in this study was 26 per group. A consideration of possible attrition was counted for 30% (Polit & Gillespie, 2009), giving the final sample size of 34 per group.
Measures
A Malay-translated Diabetic Foot Selfcare Behavior Scale (DFSBS) (Chin & Huang, 2013) and a Dietary Behavior Questionnaire (DBQ) (Pamungkas, 2015) were used in assessing foot care behavior and dietary behavior. Permission was given by the original authors to translate the DFSBS and DBQ into Malay language. The translated version of the questionnaires adopted was found to be acceptable, with Cronbach Alpha values of 0.752 (DFSBS) and 0.757 (DBQ). A checklist was used to assess foot conditions, specifically on the skin dryness, presence of calluses, heel fissures, tinea pedis, interdigital lesions, and skin cracking on the foot.
Intervention
Control group
The patient was assessed for foot care behavior, dietary behavior, fasting blood glucose, and foot condition in Week 1 as baseline data and Week 5 as comparison data. Standard care was provided by a diabetes nurse educator, as recommended by the Ministry of Health Malaysia, consisting of a face-to-face approach to delivering health education on diabetic foot care and prevention of diabetic foot ulcers together with the general management of diabetes mellitus. After the standard care was provided, the patient was allowed to carry on their day-to-day activities as usual. No assessment or intervention was provided within a five-week duration.
Intervention group
A similar assessment was carried out on the patients in the intervention group at a similar time frame (Week 1 and Week 5). The patient was included in the Diabetic Care Self-Management Mobile Health Application Program for a 5-week duration. The Diabetic Care Self-Management Mobile Health Application (Diabetic Care App) was developed by the researcher. The app was validated by a team of experts with a good content validity score (1.00) during the validity assessment by the researcher (Firdaus et al., 2022). The Diabetes Care App, developed for Android user phones, has six main menus: Foot Care Activity, Foot Care Exercise, Foot Care Records, Foot Care Tips, Diabetic Food Plate, and Food Calorie Tips. Each menu will direct the user to the videos, figures, and content related to each section. The details of the app can be read at https://doi.org/10.33546/bnj.2127.
The intervention program was started commencing after the first assessment was conducted. The activities conducted during the program consist of a two-hour face-to-face session on diabetic foot care and general management of diabetes mellitus, delivered by the researcher. A learning contract was produced during the session, and a Diabetic Care App was downloaded on the patient’s cell phone. The patient was taught the features of the app, such as the method of use and data entry regarding the foot care activities carried out. A WhatsApp group was created for discussion and facilitated by a diabetes nurse educator.
From Week 2 to Week 4, the patient performed foot care activities independently in their setting. A daily reminder was sent to the patient to engage in foot care activities and enter the data into the app. Continuous monitoring was carried out during the program conducted. The learning contract was reviewed on Day 7 each week to see the achievement. If the learning contract was unachievable on that week, it was carried forward to the following weeks until it was achieved. If the patient has any concerns, they may use WhatsApp room as the medium of communication with the diabetes nurse educator. Family members were encouraged to be involved in assisting the patient in performing foot care activities and managing their daily dietary and blood glucose. The patient returned to the clinic in Week 5 for follow-up care and post-intervention assessment. All foot care activities data were collected from WhatsApp room and cloud database for further analysis.
Data Collection
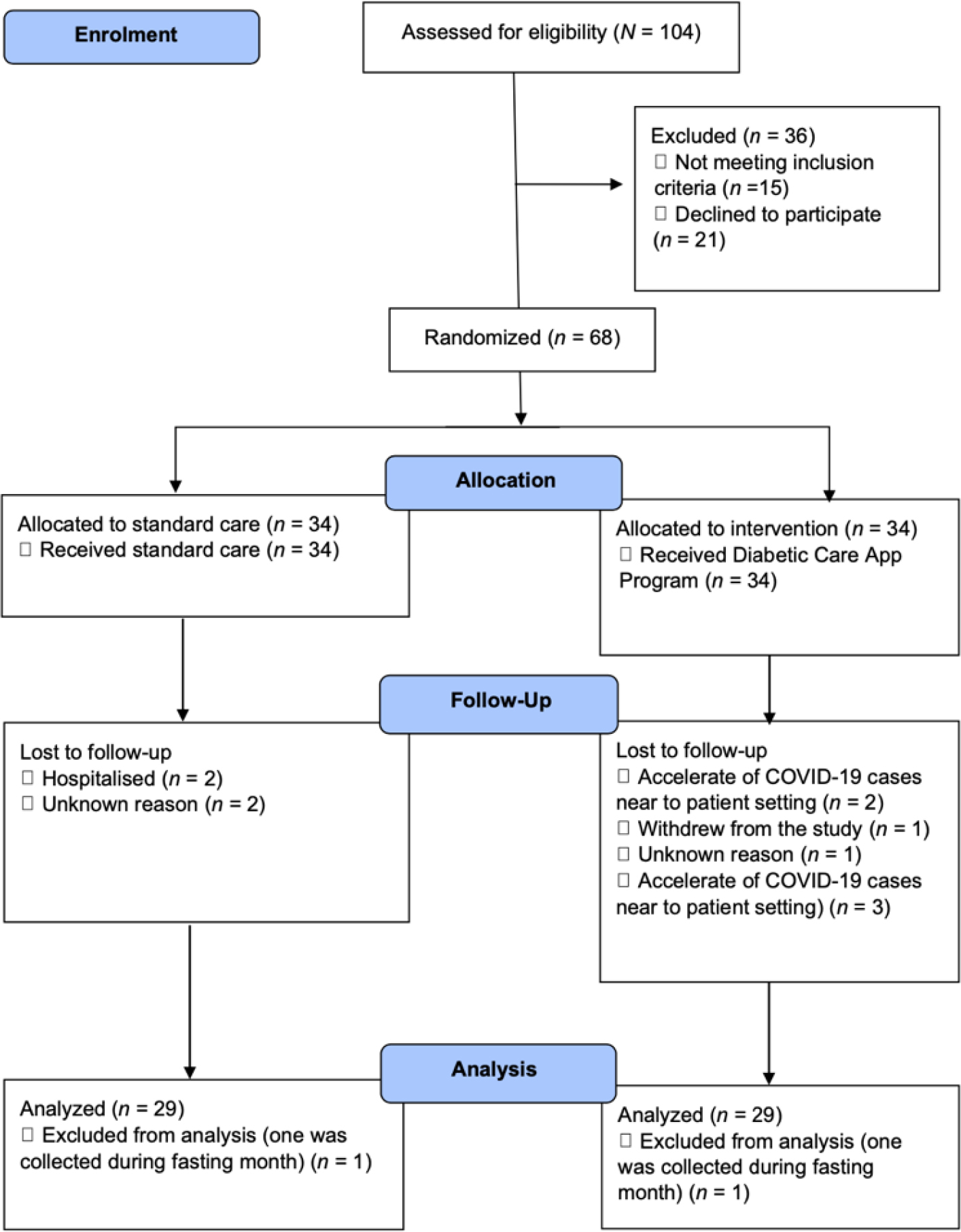
Initially, a total of 104 patient was approached and introduced to the program (N = 104). Out of 104 approached patients, 21 potential patients declined the invitation to join this study (n = 21), and 6 of the patients approached did not fulfill the inclusion criteria, such as the HbA1c level being less than 6.5% (n = 6). Written consent was taken before the screening process. The patient was then screened for risk of diabetic foot ulcer according to Inlow’s 60-Second Diabetic Foot Screen tool (Inlow, 2004). If the patient fulfilled all the inclusion criteria, the patient was invited to join this study and assigned to the groups according to Minimization Software. During the minimization process, age, gender, monthly income, and level of education were included as the potential confounding factors. The minimization software will run its process in determining the group of participants by including the confounding factors identified earlier. After the screening process, another nine patients were excluded due to having no risk for diabetic foot ulcer (stage 0) (n = 9).
A total of 68 (n = 34 in each group) patients were recruited. However, throughout the program, only 60 (n = 30 for each group) patients remained in the study. The dropout happened due to being hospitalized (n = 2 in the control group), accelerating COVID-19 cases near the patient setting (n = 2 in the intervention group), withdrawing from the study on the Day 2 enrolment (n = 1 in the intervention group) and the unknown reason why the patient did not turn up during the follow-up session (n = 1 in the intervention group and n = 2 in the control group). Hence, they were afraid to visit the clinic for follow-up and only stay home. Another 2 cases (n = 1 in each group) were excluded because the patients were assessed during Ramadhan (a fasting month for Muslims from mid-May until early June during the data collection period). During Ramadhan, the dietary behavior was slightly different compared to other months. For instance, Muslim patients can take any food from sunset (7.00 p.m. to 7.30 p.m.) to dawn (5.00 a.m. to 5.45 a.m.). Other than that, Muslim patients started to fast and did not take any food or drink during the day until sunset. Changes in dietary behavior and body metabolisms, such as body weight changes and liver glycogenolysis, might as well occur among fasting patients (Azizi, 2010) compared to the normal day. The changes in dietary behavior were expected; the patient might as well take food only two times, during breakfast and during sahur (dawn time before starting fasting), compared to a normal day, at least three times per day (breakfast, lunch, and dinner). Hence, these two patients were excluded from the data analysis. Thus, the final number of participants recruited was 58. The summary of data collection can be seen in Figure 1.
Data Analysis
There was 11.8% (n = 4 in each group) of missing data presented in this data, and another 2.9% (n = 1 in each group) was excluded due to explained reasons in the data collection section. All of the missing data were excluded from the analysis as per the protocol analysis suggested, together with the omitted case with reason. Per protocol analysis was conducted in this study to get precise and accurate results. Per protocol, the analysis will only include those who strictly adhered to the protocol, which can estimate the efficacy of the intervention based on those who completed the study (Ranganathan et al., 2016; Tripepi et al., 2020).
Data were analyzed using SPSS version 22. The data were checked for normality and assumption required before being run for either parametric or non-parametric tests. The data then matched the appropriate test accordingly. In the comparison of the pretest-posttest within the group, a paired t-test was conducted for foot care behavior, dietary behavior, fasting blood glucose, and foot conditions in the intervention group, while only the foot condition was for the control group. A non-parametric test of Wilcoxon signed rank was used in comparing the pretest-posttest effect on foot care behavior, dietary behavior, and fasting blood glucose in the control group. Meanwhile, in comparing the effect between the groups, MANCOVA analysis was used on foot care behavior, dietary behavior, and foot condition. Mann-Whitney U test was used to compare fasting blood glucose between groups.
Ethical Considerations
The study was approved by the Social and Behavioral Sciences Institutional Review Board, Faculty of Nursing, Prince of Songkla University, Hat Yai, Thailand (Certificate No: PSU IRB 2019 – NSt 017) and Medical Research Ethics Committee, Ministry of Health Malaysia (NMRR-19-3168-51578(IIR). The study was registered on 7 February 2020, with Clinical Trial Registration: NCT04260100 (https://clinicaltrials.gov/ct2/show/NCT04260100).
Results
Sociodemographic Characteristics of the Patients
A total of 58 patients completed the study with equal numbers in each group (n = 29): the intervention and control groups. The mean age of the patients was 50.03 (SD = 8.03) and 57.59 (SD = 7.18) in the intervention and control groups. The age range of the patients was as young as 34 and 44 years old and as old as 64 and 65 years old in the intervention and control group. The majority of the patients in the intervention group were female (70%), of Malay ethnicity (93.3%), educated to a secondary level (82.8%), and had a family history of diabetes mellitus (86.2%). Meanwhile, 65.5% of the patients did not work in the public sector. The patients were noted to have an almost evenly distribution of having (48.3%) and not having (51.3%) prior knowledge of foot care. The source of knowledge received was mainly from the clinic (66.7% in the intervention group and 100% in the control group) (Table 1).
| Variables | Intervention group (n = 29) | Control group (n = 29) | Statistic value | p-value | ||
|---|---|---|---|---|---|---|
| n | % | n | % | |||
| Sociodemographic Characteristics | ||||||
| Age (year) | Mean = 50.03; SD = 8.03 (Min = 34, Max = 64) | Mean = 57.59; SD = 7.18 (Min = 38, Max = 65) | -3.774a | <0.001* | ||
| Gender | 0.76b | 0.782 | ||||
| Male | 9 | 31.0 | 11 | 37.9 | ||
| Female | 20 | 69.0 | 18 | 62.1 | ||
| Ethnicity | 1.000c | |||||
| Malay | 27 | 93.3 | 27 | 93.3 | ||
| Non-Malay | 2 | 6.7 | 2 | 6.7 | ||
| Education | 1.000c | |||||
| Secondary and below | 24 | 82.8 | 25 | 86.2 | ||
| More than secondary | 5 | 17.2 | 4 | 13.8 | ||
| Occupation | 2.354b | 0.125 | ||||
| Public sector employees | 10 | 34.5 | 4 | 13.8 | ||
| Not employed in the public sector | 19 | 65.5 | 25 | 86.2 | ||
| Monthly income (MYR) | Mean = 2582.76 SD = 1949.92 (Min = 500, Max = 8000) | Mean = 1517.24 SD = 2029.83 (Min = 300, Max = 10000) | 2.039a | 0.046* | ||
| Duration of diabetes (year) | Mean = 8.76; SD = 6.09 (Min = 2, Max = 22) | Mean = 8.90; SD = 5.69 (Min = 2, Max = 23) | -0.089a | 0.929 | ||
| Family history of diabetes | 12.376b | <0.001* | ||||
| Yes | 25 | 86.2 | 11 | 37.9 | ||
| No | 4 | 13.8 | 18 | 62.1 | ||
| Prior knowledge of foot care | 0.640b | 0.424 | ||||
| Yes | 14 | 48.3 | 10 | 34.5 | ||
| Clinic | 9 | 64.3 | 10 | 100.0 | ||
| Other than Clinic | 5 | 35.7 | - | - | ||
| No | 15 | 51.7 | 19 | 65.5 | ||
| Health Status | ||||||
| Stage risk of foot ulcers | 0.449b | 0.503 | ||||
| 1 | 22 | 75.9 | 25 | 86.2 | ||
| 2 | 7 | 24.1 | 4 | 13.8 | ||
| HbA1c (mmol/L) | Mean = 9.138; SD = 1.956 (Min = 6.90, Max = 13.20) | Mean = 9.151; SD = 2.237 (Min = 7.00, Max = 15.70) | 0.025a | 0.980 | ||
| Co-morbidity | 0.423d | |||||
| No co-morbidity | 5 | 17.2 | 2 | 6.9 | ||
| At least 1 co-morbidity | 24 | 82.8 | 27 | 93.1 | ||
| Medication | 0.423d | |||||
| Only diabetics | 5 | 16.7 | 2 | 6.9 | ||
| Diabetics & others | 24 | 82.8 | 27 | 93.1 | ||
| 10g monofilament testing sites | ||||||
| Left foot | 0.300e | |||||
| 0 site | 6 | 20.7 | 2 | 6.9 | ||
| 1-3 sites | 18 | 62.1 | 23 | 79.3 | ||
| 7 -10 sites | 5 | 17.2 | 4 | 13.8 | ||
| Right foot | 0.000b | 1.00 | ||||
| 0 site | 6 | 20.7 | 5 | 17.2 | ||
| 1-3 sites | 23 | 79.3 | 24 | 82.8 | ||
| Vibration test | 0.491d | |||||
| Yes | 29 | 100.0 | 27 | 93.1 | ||
| No | - | - | 2 | 6.9 | ||
The mean monthly income of the patients was MYR 2582.76 (SD = MYR 1949.92) and MYR 1517.24 (SD = MYR 2024.83) among both groups. The monthly income range was MYR 500 to MYR 8000 in the intervention group and MYR 300 to MYR 10000 in the control group. For the duration of diabetes, the mean duration in the intervention group was 8.67 (SD = 6.09) years, while for the control group, the mean was 8.90 (SD = 5.69) years. The shortest duration of diabetes among the patients for both groups was two years, while the longest was 22 years for the intervention group and 23 years for the control group.
There was a significant difference between groups only on age (p <0.01), monthly income (p <0.05), and family history (p <0.01) out of all socio-demographic characteristics assessed (gender, ethnicity, occupation, level of education, duration of diabetes and prior knowledge on foot care).
Health Information and Foot Conditions
The mean level of HbA1c among the patients in the intervention group was 9.138 (SD = 1.956) mmol/L, while an approximate 9.151 mean reading (SD = 2.237) was noted among patients in the control group. The lowest reading was 6.90 mmol/L for the intervention group, while 7.00 mmol/L was the reading for the control group. The highest reading showed a 2.50 mmol/L lower in the intervention group than 15.70 mmol/L in the control group. The majority of the patients in both groups presented with Stage 1 risk for foot ulcers, comorbidity, and having more than one type of medication. The patients showed that they have at least 1 to 3 sites of loss of sensation after 10g monofilament testing was carried out either on the left or right foot. However, when vibration testing was performed, only 6.9% of patients in the control group were not able to detect the vibration. No significant difference was noted when comparing the groups on patients’ health information and foot conditions (Table 1).
Comparison of foot care behavior, dietary behavior, fasting blood glucose, and foot conditions between pretest and posttest in intervention and control groups
There was an improvement in foot care behavior, dietary behavior, and foot conditions among both groups when a comparison at the pretest and posttest was conducted. Significance difference in the intervention group was noted on foot care behavior (t = -18.941, p <0.01), dietary behavior (t = -5.718, p <0.01) and foot conditions (t = 4.894, p <0.01) while in the control group as follow: foot care behavior (Z = -4.707, p < 0.01), dietary behavior (Z = -3.183, p < 0.01) and foot condition (t = 4.01, p <0.01). However, fasting blood glucose showed no significant difference in both groups (intervention, Z = 0.110, p = 0.913; control group, Z = -0.729, p = 0.466) when comparing the mean score at the pretest and posttest (Table 2).
| Variable | Pretest (n = 29) | Posttest (n = 29) | ta | p-value | ||
|---|---|---|---|---|---|---|
| Mean | SD | Mean | SD | |||
| Intervention group | ||||||
| Foot care behavior | 15.760 | 4.290 | 31.620 | 3.278 | -18.941 | <0.001* |
| Dietary behavior | 51.590 | 10.172 | 62.030 | 15.518 | -5.718 | <0.001* |
| Fasting blood glucose (mg/dl) | 158.076 | 56.313 | 157.193 | 57.313 | 0.110 | 0.913 |
| Foot condition | 2.140 | 1.407 | 1.480 | 0.911 | 4.894 | <0.001* |
| Control group | ||||||
| Foot condition | 2.520 | 1.056 | 2.000 | 0.964 | 4.050 | <0.001* |
| Variable | Pretest (n = 29) | Posttest (n = 29) | Zb | p-value | ||
| Median | IQR | Median | IQR | |||
| Control group | ||||||
| Foot care behavior | 14.170 | 4.420 | 22.000 | 9.500 | -4.707c | <0.001* |
| Dietary behavior | 50.000 | 13.380 | 53.000 | 17.180 | -3.183c | <0.001* |
| Fasting blood glucose (mg/dl) | 137.000 | 44.750 | 133.667 | 52.350 | -0.729d | 0.466 |
Comparison of foot care behavior, dietary behavior, fasting blood glucose, and foot conditions between the groups at the pretest and posttest
Comparisons of pretest scores were performed between the intervention and control groups. However, no significant differences were noted in foot care behavior (Z = -0.969, p = 0.332), dietary behavior (Z = -0.1872, p = 0.852), fasting blood glucose (Z = 0.389, p = 0.697) and foot conditions (t = -1.161, p = 0.251) (Table 3).
| Variable | Intervention group (n = 30) | Control group (n = 30) | Za | p-value | ||
|---|---|---|---|---|---|---|
| Mean rank | Sum of ranks | Mean rank | Sum of ranks | |||
| Pretest | ||||||
| Foot care behavior | 31.640 | 917.50 | 27.360 | 793.50 | -0.969 | 0.332 |
| Dietary behavior | 29.910 | 867.50 | 29.090 | 843.50 | -0.187 | 0.852 |
| Fasting blood glucose (mg/dl) | 30.360 | 880.50 | 28.640 | 830.50 | -0.389 | 0.697 |
| Variable | Intervention group (n = 30) | Control group (n = 30) | tb | p-value | ||
| Mean | SD | Mean | SD | |||
| Pretest | ||||||
| Foot care condition | 2.140 | 1.407 | 2.520 | 1.056 | -1.161 | 0.251 |
Conversely, a significant finding in posttest analysis when comparing foot care behavior (F = 30.374, p <0.01, Wilks’ Λ = 0.628, partial η2 = 0.364) and dietary behavior (F = 7.533, p <0.05, Wilks’ Λ = 0.628, partial η2 = 0.124) between groups was noted after controlling for age, monthly income, and family history of the patients. While fasting blood glucose (Z = -0.381, p = 0.703) and foot conditions (F = 0.995, p = 0.323, after controlling for age, monthly income, and family history of the patients) showed no significant difference between the groups (Table 4 and Table 5).
| Source of variance | Sum of square | df | Mean square | F | p-value | ŋ2p | MI | Mc | |
|---|---|---|---|---|---|---|---|---|---|
| Foot care behavior | Main effect: Group | 671.989 | 1 | 671.989 | 30.374 | <0.001* | 0.364 | 32.40 | 23.56 |
| Covariates | |||||||||
| Age | 68.429 | 1 | 68.429 | 3.098 | 0.084 | ||||
| Monthly income | 0.076 | 1 | 0.076 | 0.003 | 0.953 | ||||
| Family history | 9.594 | 1 | 9.594 | 0.434 | 0.513 | ||||
| Dietary behavior | Main effect: Group | 1483.501 | 1 | 1483.501 | 7.533 | 0.008* | 0.124 | 65.14 | 51.60 |
| Covariates | |||||||||
| Age | 1020.850 | 1 | 1020.850 | 5.184 | 0.027 | ||||
| Monthly income | 25.548 | 1 | 25.548 | 0.130 | 0.720 | ||||
| Family history | 223.246 | 1 | 223.246 | 1.134 | 0.292 | ||||
| Fasting blood glucose (mg/dl) | Main effect: Group | 0.858 | 1 | 0.858 | 0.955 | 0.323 | 0.018 | 1.583 | 1.899 |
| Covariates | |||||||||
| Age | 0.336 | 1 | 0.133 | 0.154 | 0.696 | ||||
| Monthly income | 2.181 | 1 | 2.181 | 2.530 | 0.181 | ||||
| Family history | 0.896 | 1 | 0.896 | 1.039 | 0.313 | ||||
Note:
| Variable | Intervention group (n = 29) | Control group (n = 29) | Z | p-value | ||
|---|---|---|---|---|---|---|
| Mean rank | Sum of ranks | Mean rank | Sum of ranks | |||
| Posttest | ||||||
| Fasting blood glucose (mg/dl) | 30.340 | 880.00 | 28.660 | 831.00 | -0.381 | 0.703 |
Discussion
The findings of this study show the mean scores for foot care behavior and dietary behavior were significantly higher in the pretest-posttest comparisons and between-group comparisons after controlling for age, monthly income, and family history of diabetes. The findings of this study supported the concept of self-management and mobile health employed in the intervention program. Even though similar concepts were used in other studies (Ahn et al., 2016; Ramadas et al., 2018), there is little evidence showing the integration of self-management with mobile health. The difference in this study is the integration of self-management with a smartphone mobile application rather than the use of a web-based application or telehealth.
The significant findings in the pretest and posttest comparison in this study are comparable to other studies on foot care behavior (Borges & Ostwald, 2008; Nguyen et al., 2019), dietary behavior (Kim et al., 2015; Sittig et al., 2020) and foot condition (Nguyen et al., 2019). This study duration was conducted for five weeks, whereas other studies ranged from 9 weeks to 6 months duration (Dincer & Bahçecik, 2021; Kilic & Karadağ, 2020; Nguyen et al., 2019; Ramadas et al., 2018; Sittig et al., 2020). Hence, it shows that a shorter study duration may improve foot care behavior, dietary behavior, and foot conditions.
In addition, a two-hour health education session was conducted at the initial program for the intervention group. Relevant foot care skills were taught together with the use of the Diabetic Care App, providing appropriate training to help the patient engage better in self-managing their condition. It is aligned with the Trans-Theoretical Model, which explains that a patient starts to explore the required behavior as a preparation stage before beginning to act (Prochaska & Velicer, 1997).
The installation of the Diabetic Care App on the patient’s phone was helpful as a source of referral in the patient’s setting. As stated in Social Learning Theory, a mediational process consists of attention, retention, reproduction, and motivation that may occur before human behavior changes (Bandura, 1969). The use of the mHealth intervention assists the patient in paying attention to their diabetes care and, therefore, creates good self-awareness of their self-managing conditions (Marcolino et al., 2018). Furthermore, the accessibility of verified information was provided in the app, which serves as a trustable source of information for patients with diabetes. Hence, the use of the app was proven able to improve foot care behavior, dietary behavior, and foot condition as other studies conducted by Dincer and Bahçecik (2021), Kilic and Karadağ (2020), and Ramadas et al. (2018).
In addition, the existence of a WhatsApp group as a room for discussion and method of monitoring for the patient may promote clients’ self-managing of the condition. Even though the diabetes nurse educator was not physically available, through the WhatsApp room, the patient still could reach him. As such, continuity of care was presented throughout the study of the period. Indirectly, it may have initiated the self-management process since the patient was aware that social support was there when they needed it. A similar situation is presented in the study of Dincer and Bahçecik (2021), Kilic and Karadağ (2020), and Ramadas et al. (2018). This is consistent with IFSMT, which includes social support as part of the theory (Ryan & Sawin, 2009). Besides, WhatsApp is well utilized as the main internet-based texting platform in Malaysia and the highest among Malaysians for day-to-day, social, and professional activities (Kemp, 2015).
The integration of the learning contract in the intervention program might as well be catalyzed for the self-management of diabetes care. Continuous monitoring via learning contract assists the patient in acquiring self-management in their daily routine, which is aligned with the Self-Management Model, which explains that self-management revolves around self-monitoring, self-evaluation, and self-reinforcement that may occur continuously (Kanfer & Gaelick-Buys, 1991). A mutual relationship between the diabetes nurse educator and the patient might contribute to patient engagement in self-management activities (King, 1992; Molina-Mula & Gallo-Estrada, 2020).
The results are in line with other studies on foot care behavior (Dincer & Bahçecik, 2021; Kilic & Karadağ, 2020), dietary behavior (Ramadas et al., 2018), while Kebede and Pischke (2019) study found there was no significant difference in specific diets, but significant difference was noted in the general diets of patients when a comparison was made between users and non-users of a diabetes app in their study. The different designs of the studies might explain the differences in findings with Kebede and Pischke (2019). Ramadas et al. (2018) conducted an intervention study, whereas Kebede and Pischke (2019) used surveys to see the difference between users and non-users of the diabetes apps.
Fasting blood glucose showed no significant difference in the pretest-posttest and group comparison. The finding of this study is similar to Rossi et al. (2013), who showed no significant difference between the pretest and posttest in the intervention group on fasting blood glucose. This may happen due to the complex process of the human body, which requires various internal and external factors to regulate its physiology. Health outcomes (fasting blood glucose and foot condition) may require a longer period before changes can be detected. Various factors might interfere with changes, such as comorbidity and medication use (Wami et al., 2013). To explain this, most of the patients enrolled in this study had at least one comorbidity and were on more than one type of medication. These factors might have impaired the possibility of detecting fasting blood glucose changes and foot condition improving significantly.
The findings on fasting blood glucose in this study contradict Hooshmandja et al. (2019), who found a significant difference in pretest-posttest and between-group comparisons after three months of their mobile health intervention. However, this study’s finding aligns with Ramadas et al. (2018), which found no significant difference in fasting blood glucose between the intervention and control groups in their six-month web-based dietary intervention for patients with type 2 diabetes mellitus.
Similarly, for foot conditions, the findings from previous studies contradict this study’s findings. Kilic and Karadağ (2020) found that the foot condition of intervention group patients was better, i.e., they had lower scores for cracked/dry skin and inappropriate footwear than the control group. Meanwhile, Nguyen et al. (2019) noted that a lower proportion of patients in the intervention group developed diabetic foot skin dryness, cracks, and corns/callouses than in the control group. Both Kilic and Karadağ (2020) and Nguyen et al. (2019) conducted their studies for longer than five weeks (6 months and 24 months, respectively). Hence, a longer study duration may explain the positive findings for foot conditions observed in their studies.
Even though this study was conducted during the Conditional Movement Control Order (CMCO) period imposed to limit the spread of COVID-19, the findings for behavioral modification (foot care behavior and dietary behavior) are similar to other earlier studies. However, significant results (foot care behavior, dietary behavior, and foot condition) were also noted among the control group during the pretest-posttest comparison. In the control group, the patients received standard care, which consisted of face-to-face and one-to-one health education during visits by the diabetes nurse educator in charge. Therefore, the patient had exposure to and information on diabetic care management. During CMCO, patients are mostly stationed in their own homes, as instructed by the Malaysian government, due to COVID-19. Knell et al. (2020) found that positive health behavior increased during stay-at-home orders during the COVID-19 situation due to more time being available (42%) and health concerns (15.1%). Hence, these two factors might explain the significant differences among the control group in the pretest-posttest comparison in this study.
Changes in dietary behavior were also noted during CMCO. The dietary behavior among Malaysians changed during the stay-at-home order in terms of increased frequency of eating (46.5%), increased sugar-sweetened drink intake (27.7%), and increased fast/instant food intake (18.1%) compared with usual (Ithnain et al., 2020). Thus, it might explain why there were no significant differences in fasting blood glucose at the pretest and posttest comparison.
Limitations of the Study
There are two limitations identified in this study, namely, the limitation of sampling and the limitation of the program. In the limitation of sampling, the sample size of this study is small (n = 58). Even though the sample size was calculated according to previous literature, the study sample was only 58 in total due to attrition (14.7 %). However, the sample size calculated for this study had already made provision for up to 30% drop-out. Thus, the total sample size gathered was considered sufficient for the analysis. Besides, the data collection was conducted during the COVID-19 pandemic. As such, many patients agreed to join in the earlier phase but refused later. Some of the enrolled patients declined to come to follow-up sessions due to the acceleration of COVID-19 cases close to their homes. Thus, patients who were absent during follow-up sessions were not included in the analysis. In addition, the study was conducted at only one site, which poses a risk of contamination, although a schedule was provided for each group of patients. Moreover, the findings cannot be generalized to the whole Malaysian population. Lastly, due to the COVID-19 pandemic, the individual face-to-face sessions with the patients were only able to be conducted within two hours as the researcher needed to abide by the 3Cs recommendation (avoid crowded places, confined spaces, and close conversation) of the Malaysian Ministry of Health.
While the limitation of the program is related to the Diabetic Care App. The first problem was regarding the process of installing the Diabetic Care App. Sometimes, installation took a long time, and the app could not be downloaded through the WhatsApp invitation. However, the diabetes nurse educator helped with the installation process through the ShareIt application and by sharing via Bluetooth. The patients ensured that the application could be used before joining the workshop session on Day 1. Moreover, in the first few days after installing the Diabetic Care App onto the patients’ phones, the patients seemed to have some difficulty using the application. However, the patients were monitored by the research assistant during the intervention period so that they were able to use the app.
In addition, the practice of foot care behavior and dietary modification could not be observed directly. Yet the research assistant followed up with the patients via the WhatsApp group by sending reminders daily. Every week, there was a learning contract review session. Thus, the patients always communicated any problems that had arisen to the research assistant. Furthermore, the patients were asked to perform self-reports of each activity using the Diabetic Care App. This application was linked to a cloud database. The researcher was able to monitor the foot care activities carried out by each patient. Lastly, the Diabetic Care App is an application that is only compatible with the Android operating system. Therefore, iPhone and non-Android phone users were not invited to this study.
Implications to the Nursing Practice
This study provides insight into the usefulness of mobile health as an alternative to health promotion and prevention approaches. In addition, it is a helpful tool for self-managing chronic conditions (diabetes mellitus), provided with guidance by a trained nurse. The study showed that mobile health apps can assist the nurse in reaching the client virtually and remotely. In the study, the client with diabetes mellitus was able to access the care in their setting and communicate via the app with the health care provider. Indirectly, continuity of care is provided to the client remotely. Furthermore, the app offers firsthand information to the client. Hence, the app can be a referral source with guided information by the nurse rather than receiving it from untrustworthy sites.
Conclusion
This study’s findings supported the use of the Diabetic Care App in improving foot care behavior, dietary behavior, and foot condition of uncontrolled diabetes mellitus clients in the northern region of Malaysia. Improvement in foot care behavior and dietary behavior was shown in this study during the pretest-posttest and between-group comparison. This study shows that the Diabetes Care App is appropriate to be used when performing self-management in a patient’s setting. The findings of this study emphasize that mobile health could be translated into care delivery systems. Additionally, it is useful for data gathering as well. The application of mobile health can help widen the scope of care, focusing on home care and remote and virtual care. The positive findings of this study should be an initial step towards translating technology as an agent for behavior modification in health care. This study proved that a mobile health application is a viable alternative method for care delivery.