









Background
Suicide has become an increasingly serious public health problem since the outbreak of the COVID-19 pandemic, which originated in China at the end of 2019 (Sher, 2020a) and spread rapidly worldwide. As of 2 July 2022, there have been 87,407,521 COVID-19 cases and 1,013,261 deaths related to COVID-19 infection worldwide (Centers for Disease Control and Prevention, 2022). In Thailand, there have been 4,525,269 cases and 30,664 deaths (World Health Organization, 2022). As a result, due to the pandemic, people’s suicidal tendencies are increasing (Banerjee et al., 2021; Sher, 2020b; Standish, 2021). Several factors have been associated with the higher suicide rate during the current pandemic, including suffering, anxiety, fear of infection, depression, insomnia, social isolation, uncertainty, stress, stigma, and financial problems (Elbogen et al., 2021; Qin & Mehlum, 2021). A cross-sectional study that examined suicidal risk in the Columbian population during the COVID-19 lockdown in Columbia found that 7.6% of the sample were at high risk of suicide due to factors associated with the COVID-19 pandemic, such as high perceived pandemic-related stress, depression, and insomnia (Caballero-Domínguez et al., 2022). A previous study also reported that suicidal and self-harm thoughts during the COVID-19 pandemic were correlated with COVID-19-related stress, loneliness, and financial problems (Elbogen et al., 2021).
A study on the mental health of the Thai people during the pandemic reported that 75.35% felt stressed and extremely worried and that 72.95% had bad feelings and experienced despair (Suondusitpoll, 2021). Another study, particularly on the stress levels of the Thai people after the first wave of the COVID-19 pandemic, revealed that most of the study participants (13.9%) had the highest stress level (Ruksee et al., 2021). In addition, a recent study on the stress levels of people in villages under lockdown due to the COVID-19 outbreak revealed a moderate stress level on average (36.8%) caused by low income due to unemployment (44.80%) or unprofitable productivity (23.20%) (Suttipun & Intarangkul, 2022). Studies have shown that employment challenges and stressful life events, in addition to anxiety sensitivity and other factors, may cause suicidal risk (Allan et al., 2021; Chaniang et al., 2022; Choompunuch et al., 2021). This risk can be found in individuals who are likely to attempt suicide and can affect their family members, relatives, and other close ones. Moreover, it has enormous social and economic effects unless there is an effective system for caring for at-risk groups by empowering those providing care for them.
Suicide prevention and resolution in Thailand are continuously being carried out by the Department of Mental Health. According to the World Health Organization, the suicide rate can be reduced by identifying people at risk of suicide, providing them with support and assistance, and seeking to prevent suicide (World Health Organization, 2012). It can be seen from the information mentioned above that many previous studies on the suicidal risk that caused by several factors. It is unclear, however, whether stress and stress-coping behaviors among the unemployed are due to the COVID-19 pandemic in Thailand.
However, despite the continuous efforts to prevent suicide and address its rising incidence among the Thai people, the number of completed suicides is not likely to decrease. Thus, this study aimed to determine the relationships between stress, stress-coping behaviors, and suicidal risk in Thais who had become unemployed due to the COVID-19 pandemic. The study results can help inform best-practice recommendations for nursing practice and develop guidelines for promoting mental health and quality of life. Future research will help find risk groups and plan their treatment, design activities for stress reduction, and promote appropriate stress-coping behaviors for unemployed people during the COVID-19 pandemic.
Methods
Study Design
This research was a cross-sectional study implemented to determine the relationships between the stress levels, stress-coping behaviors, and suicidal risk of the unemployed in Thailand due to the COVID-19 pandemic.
Samples/Participants
A total of 447 unemployed Thai people from Chun, Dok Kham Tai, Mae Chai, and Chiang Kham, Phayao Province, Thailand, were selected using multistage sampling as study participants. The sample size was determined using G∗ power 3.1.9.7 software (Faul et al., 2007). In the study, the correlation test was used for estimating the sample size (using power = 0.85, alpha = 0.05 two-tailed, effect size = 0.15); therefore, the minimum sample size was calculated to be 396. The sample size increased to 447 participants. Participants selected for the study were: (1) 18 years or above, (2) Thais who had become unemployed due to the COVID-19 pandemic, (3) willing to participate in the research, and (4) capable of completing the questionnaire themselves. Unemployed individuals who could not read the Thai language and had been diagnosed with a mental disorder were excluded from the study.
Instruments
Questionnaires were used as instruments in the present study. Permission to use them was obtained from their owners, and all the questionnaires were tested and examined by three experts for content validity and reliability.
Perceived Stress Scale (PSS), developed by Cohen et al. (1983), particularly the original Thai version of Mingkuan (1999), was used. It consists of 14 multiple-choice items. The respondents indicate their responses based on a 4-point scale, where 4 = “strongly agree,” 3 = “agree,” 2 = “disagree,” and 1 = “strongly disagree.” PSS was used for questions concerning the respondents’ feelings about various situations during their unemployment in the past month due to the COVID-19 pandemic. PSS scores can range from 14 to 56; they were interpreted as follows: low perceived stress (score ≤ 18), moderate perceived stress (score 18.01–37.00), and high perceived stress (score 37.01–56.00). The Cronbach’s alpha coefficient in this study was 0.84.
Jalowiec Coping Scale (JCS), developed by Jalowiec et al. (1984) and translated into Thai by Mingkuan (1999), was used. It consists of 36 multiple-choice items with a 4-point response scale, where 4 = “strongly agree,” 3 = “agree,” 2 = “disagree,” and 1 = “strongly disagree.” We used JCS to assess the frequency of the participants’ use of coping strategies and the participants’ stress-coping behaviors. We divided it into three types of stress-coping behaviors, as follows: (1) problem confrontation (13 items), with scores ranging from low (5–25 points) to moderate (26–45 points) and high (46–65 points); (2) emotional management (9 items), with scores ranging from low (5.00–18.33 points) to moderate (18.34–31.66 points) and high (31.67–45.00 points); and (3) problem alleviation (14 items), with scores ranging from low (5.00–26.67 points) to moderate (26.68–43.35 points) and high (43.36–70.00 points). The Cronbach’s alpha coefficient in this study was 0.93.
Psychiatric Inpatient Suicide Risk Assessment (PISRA) was also used in the present study, particularly the Thai version (Psychiatric Inpatient Suicide Risk Assessment) by Sonthe et al. (2020). It consists of 12 multiple-choice items with a 4-point response scale, where 4 = “strongly agree,” 3 = “agree,” 2 = “disagree,” and 1 = “strongly disagree.” Suicide risk is categorized into four levels: high (≥ 15 points), moderate (7–14 points), low (1–6 points), and normal or no risk (0 point). The Cronbach’s alpha coefficient in this study was 0.83.
Sociodemographic variables. We collected the following general data from the participants: sex, age, marital status, education level, religion, occupation, monthly income before becoming unemployed, monthly family income, income adequacy, monthly financial liabilities, family role, family relationships, medical expenses payment scheme, physical congenital disease, congenital mental disease, history of alcohol consumption, and history of suicide in the family.
Data Collection
A self-administered questionnaire was used to collect data from the participants from 1 July to 30 September 2021. It took the participants 30–40 minutes to complete the questionnaire. There was no research assistant recruited for this study.
Data Analysis
Statistical Package for Social Sciences (SPSS) version 21 was used to analyze the data. Descriptive statistics (i.e., frequency, percentage, mode, mean, and standard deviation) were used to present the data. In addition, Spearman’s correlation coefficient was used to determine the relationships between stress, stress-coping behaviors, and suicidal risk. The significance level was set at p <0.05 for all analyses.
Ethical Considerations
This study was approved by the Ethical Committee Review Board of the University of Phayao Human Ethics Committee (UP-HEC 1.3/019/64). The participants signed an informed consent form before participating in the study. The study objectives and procedures were explained to the participants. Confidentiality of the data was strictly secured.
Results
Characteristics of the Participants
As shown in Table 1, of the 447 study participants, 59.73% (n = 267) were female, 29.08% (n = 130) were 31–40 years old, 56.60% (n = 253) were married, and 30.87% (n = 138) had completed secondary school. Moreover, 98.43% (n = 440) were Buddhists, 36.91% (n = 165) were employees, 36.02% (n = 161) had a monthly income before becoming unemployed of less than US$151, 30.43% (n = 136) had a monthly family income of US$152–303, 58.39% (n = 261) had insufficient incomes, 51.68% (n = 231) had financial liabilities, 94.42% (n = 355) had financial liabilities less than US$151, 51.90% (n = 232) had the role of family member, 75.62% (n = 338) had good relationships with the other members of their families, and 56.82% (n = 254) had health insurance coverage. In addition, 79.64% (n = 356) did not have a history of physical congenital disease, 10.74% (n = 48) had hypertension, 100.00% (n = 447) had no history of mental disorders, 60.85% (n = 272) had no history of alcohol consumption, and 99.78% (n = 446) had no history of suicide in their family.
| Personal information | n | % |
|---|---|---|
| Sex | ||
| Male | 180 | 40.27 |
| Female | 267 | 59.73 |
| Age (years) | ||
| < 20 | 14 | 3.13 |
| 21–30 | 82 | 18.34 |
| 31–40 | 130 | 29.08 |
| 41–50 | 102 | 22.82 |
| > 51 | 119 | 26.62 |
| Mean = 41.74; SD = 12.26; range = 15–60 | ||
| Marital status | ||
| Single | 135 | 30.20 |
| Married | 253 | 56.60 |
| Separated | 15 | 3.36 |
| Widow | 34 | 7.61 |
| Divorced | 10 | 2.24 |
| Education level | ||
| Uneducated | 6 | 1.34 |
| Primary school | 133 | 29.76 |
| Secondary education | 138 | 30.87 |
| Vocational certificate/diploma | 65 | 14.54 |
| Bachelor’s degree or higher | 105 | 23.49 |
| Religion | ||
| Buddhist | 440 | 98.43 |
| Christian | 5 | 1.12 |
| Islam | 1 | 0.22 |
| Other (prefer not to answer) | 1 | 0.22 |
| Occupation before becoming unemployed | ||
| Private company/factory employee | 36 | 8.05 |
| Farmer | 56 | 12.53 |
| Employee | 165 | 36.91 |
| Vendor | 65 | 14.54 |
| Self-employed/business owner | 103 | 23.04 |
| Other (prefer not to answer) | 22 | 4.92 |
| Income before becoming unemployed (USD/month) | ||
| < 151 | 161 | 36.02 |
| 152–303 | 147 | 32.89 |
| 304–454 | 90 | 20.13 |
| 455–606 | 16 | 3.58 |
| > 607 | 33 | 7.38 |
| Family income (USD/month) | ||
| < 151 | 82 | 18.34 |
| 152–303 | 136 | 30.43 |
| 304–454 | 106 | 23.71 |
| 455–606 | 54 | 12.08 |
| > 607 | 69 | 15.44 |
| Income adequacy | ||
| Adequate | 186 | 41.61 |
| Inadequate | 261 | 58.39 |
| Financial liabilities | ||
| Yes | 231 | 51.68 |
| No | 216 | 48.32 |
| Amount of financial liabilities (USD/month) | ||
| < 151 | 355 | 79.42 |
| 152–303 | 54 | 12.08 |
| 304–454 | 21 | 4.70 |
| > 455 | 17 | 3.80 |
| Family role | ||
| Leader | 132 | 29.53 |
| Member | 232 | 51.90 |
| Resident | 82 | 18.34 |
| Other (prefer not to answer) | 1 | 0.22 |
| Family relationships | ||
| Poor | 0 | 0.00 |
| Quite poor | 15 | 3.36 |
| Quite good | 94 | 21.03 |
| Good | 338 | 75.62 |
| Medical expenses payment scheme | ||
| Social security | 124 | 37.78 |
| Universal coverage (30 baht for all treatments) | 254 | 56.82 |
| An agency | 6 | 1.34 |
| Person-with-disability rights | 1 | 0.22 |
| Savings | 5 | 1.12 |
| Payment through a loan | 1 | 0.22 |
| Payment by a child | 1 | 0.22 |
| Other (prefer not to answer) | 55 | 12.30 |
| History of physical congenital disease | ||
| No | 356 | 79.64 |
| Yes | 91 | 20.36 |
| Physical congenital disease | ||
| Hypertension | 48 | 10.74 |
| Diabetes | 20 | 4.47 |
| Hyperlipidemia | 10 | 2.24 |
| Allergy | 8 | 1.79 |
| Gout/osteoarthritis/another bone disease | 5 | 1.12 |
| Toxic thyroid | 3 | 0.67 |
| Heart disease | 4 | 0.89 |
| Asthma | 3 | 0.67 |
| Gastritis | 4 | 0.89 |
| Cancer | 3 | 0.67 |
| Migraine | 2 | 0.45 |
| Chronic kidney disease | 2 | 0.45 |
| Gastroesophageal reflux disease | 1 | 0.22 |
| Chronic obstructive pulmonary disease | 1 | 0.22 |
| Thalassemia | 2 | 0.45 |
| AIDS | 1 | 0.22 |
| History of mental disorder | ||
| No | 447 | 100.00 |
| Yes | 0 | 0.00 |
| History of alcohol consumption | ||
| No | 272 | 60.85 |
| Yes | 175 | 39.15 |
| Family member with a history of suicide | ||
| No | 446 | 99.78 |
| Yes | 1 | 0.22 |
Stress and Suicidal Risk Levels of the Study Participants
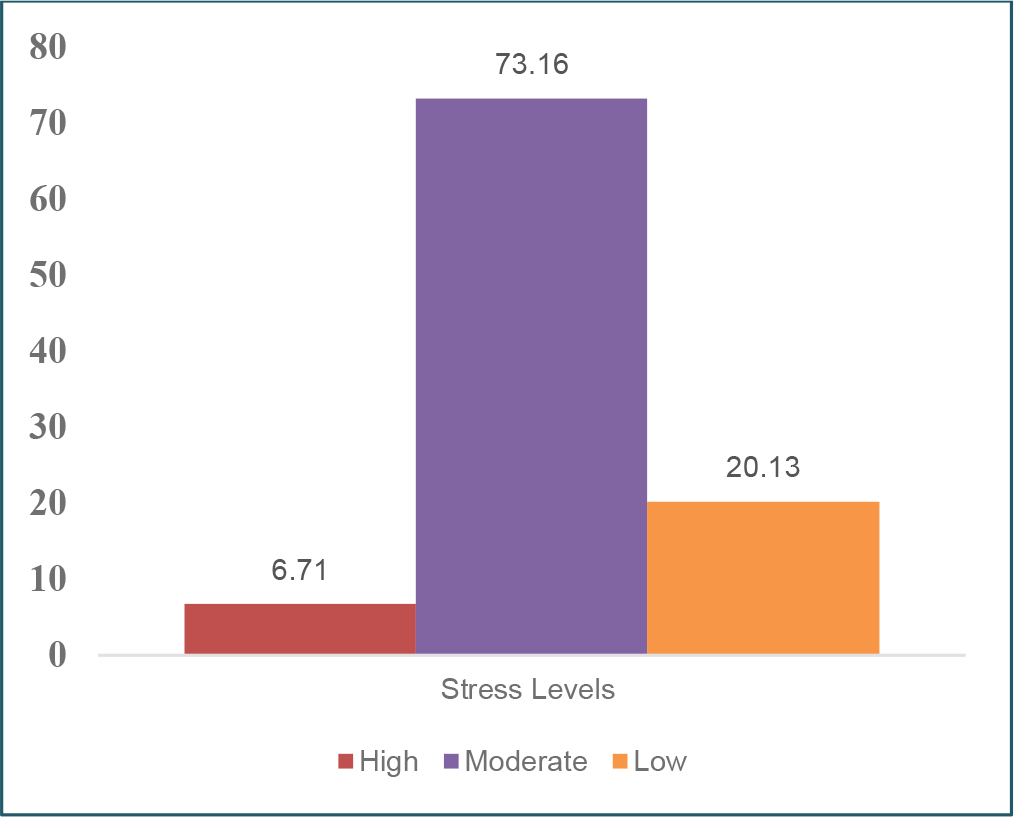
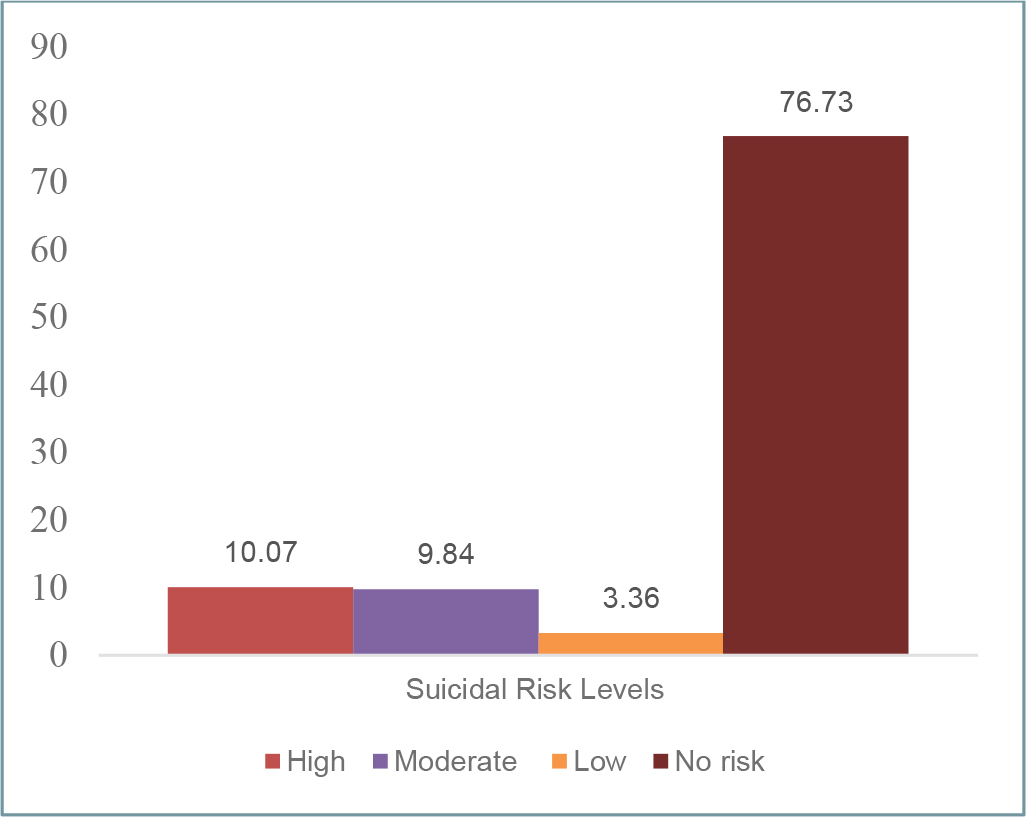
Most of the participants (73.16%) had a moderate stress level, 20.13% had a low-stress level, and 6.71% had a high-stress level (Figure 1). On the other hand, most of the participants (76.73%) had no suicidal risk, 10.07% had a high level of suicidal risk, 9.84% had a moderate level, and 3.36% had a low level (Figure 2).
Stress-Coping Behavior Levels of the Study Participants
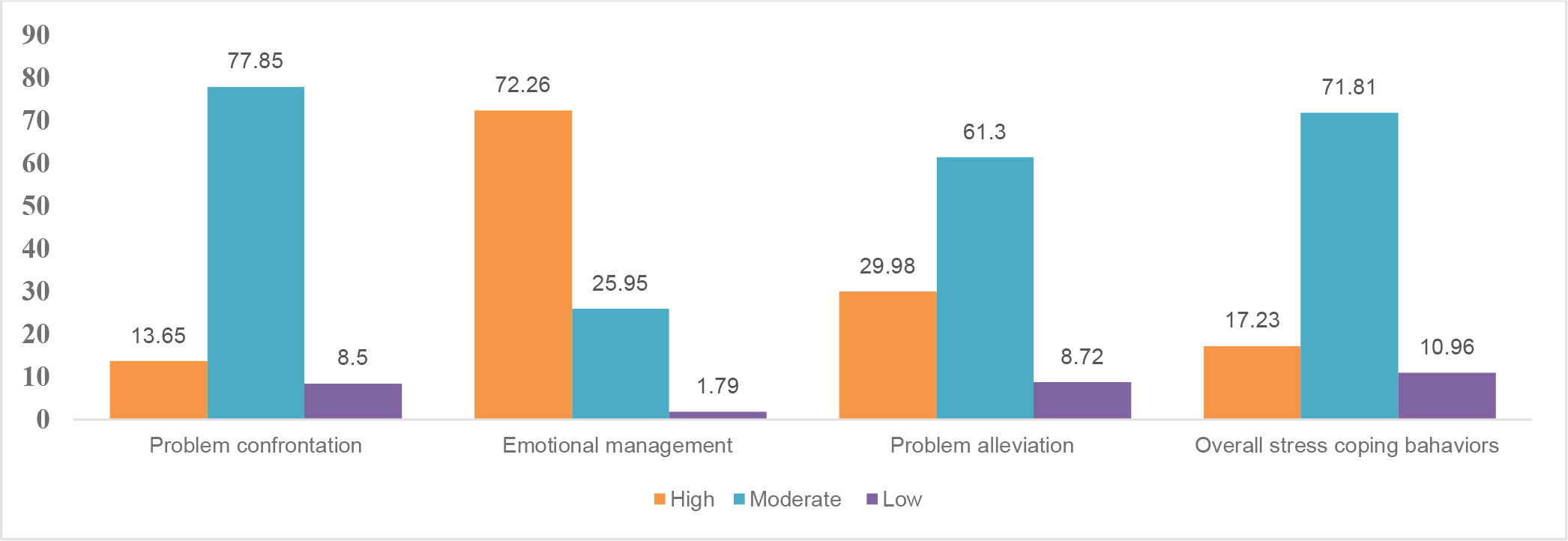
As shown in Figure 3, the overall stress-coping behavior of the participants was at a moderate level (71.81%; n = 321) when considered by component. They had moderate stress levels in terms of problem confrontation (77.85%; n = 321) and problem alleviation (61.30%; n = 274). Moreover, they had a low level of emotional management (72.26%; n = 323).
Relationships Between Stress, Stress-Coping Behaviors, and Suicidal Risk
The analysis of the relationship between stress and suicidal risk among the participants using Spearman’s correlation coefficient showed that stress was positively associated with suicidal risk at a moderate level (r = 0.305, p <0.01). In addition, the results of the analysis of the relationship between overall stress-coping behaviors and suicidal risk among the participants using Spearman’s correlation coefficient showed that stress-coping behaviors were positively associated with suicidal risk at a low level (r = 0.246, p <0.01) and that the problem confrontation, emotional management, and problem alleviation stress-coping behaviors were positively associated with suicidal risk also at a low level (r = 0.258, p <0.01; r = 0.231, p <0.01; and r = 0.186, p <0.01, respectively), as shown in Table 2.
| Variable | Suicidal risk | |
|---|---|---|
| Correlation coefficient (r) | p-value | |
| Stress | 0.305 | <0.01 |
| Stress-coping behaviors | 0.246 | <0.01 |
| Problem confrontation | 0.285 | <0.01 |
| Emotional management | 0.231 | <0.01 |
| Problem alleviation | 0.186 | <0.01 |
Discussion
The present study found that the stress levels of the participants due to the COVID-19 pandemic were moderate on average (73.16%). It thus demonstrated the impact of unemployment on mental health-related stress among unemployed Thais. Unless the unemployed were adequately supported, they felt isolated after being separated from society. Due to their insufficient incomes (58.39%) and financial liabilities (55.93%), they could develop stress. The results of the present study were different from those of another study on the Thai people by Ruksee et al. (2021); they found that the stress levels of the Thai people after the first wave of the COVID-19 pandemic were at the lowest level (56.20%). In addition, the present study was different from that by Suttipun and Intarangkul (2022), who found that the Thai people residing in villages that were placed under lockdown due to the third to fourth waves of the COVID-19 pandemic had the lowest stress level (52%). This is consistent with the results of a study conducted in Bangladesh, which indicated that economic problems, adversity, and food crises result in stress; 85.60% of the people of Bangladesh have experienced stress due to the COVID-19 pandemic (Islam et al., 2020).
The overall stress-coping behaviors of the sample were at a moderate level. This may be because, as in the study mentioned above, the unemployed Thais in the present study attempted to manage their moderate stress levels by coping with their problems. As a result, most of them applied problem alleviation and confrontation at moderate to high levels (91.18% and 88.59%, respectively), while 29.98% and 11.19%, respectively, employed problem alleviation and problem confrontation at high levels. Therefore, it can be said that the unemployed Thais in the present study used a problem-based approach to cope with their stress rather than an emotional one. This is consistent with the theory of Lazarus and Folkman (1987), which states that the unemployed will apply stress-coping behaviors during the COVID-19 pandemic based on their assessment and will attempt to reduce their stress by alleviating their problems using various techniques. However, the nature of the participants’ problems is such that they cannot directly solve them. As a result, the participants shifted to problem confrontation; that is, they analyzed the issues that were causing them stress and came up with comprehensive solutions using their learning, conflict resolution, and time management skills and choosing the best one among such solutions (Mousteri et al., 2019).
A recent study found that the participants had suicidal risk (10.07%). Most of them were unemployed, of working age (18–60 years old), and employees (36.91%). During the second wave of the COVID-19 pandemic, when the study participants were laid off, they needed to return to their hometowns despite having financial liabilities (51.68%). In addition, they were family members or leaders and had congenital diseases and a history of alcohol consumption. All these factors led to higher stress if their stress-coping behaviors depended on their abilities and support resources or opportunities to deal with their situation (McGee et al., 2021). If the unemployed, due to the COVID-19 pandemic, assessed their stress without a cognitive evaluation process or applied improper stress management to reduce their stress, severe stress could develop, which is a factor leading to suicidal risk. Similar to previous studies in many countries, the present study revealed that the following factors could be associated with suicidal risk during the COVID-19 pandemic: unemployment, social isolation, uncertainty, chronic stress, economic problems, and financial stress (Banerjee et al., 2021; Elbogen et al., 2021; Sher, 2020b). The suicide risk may depend on the severity of the situation one is in and on one’s characteristics. In addition, a previous study also reported that a high risk of suicide was found in 7.60% of its participants during the lockdown in Colombia due to the COVID-19 pandemic (Caballero-Domínguez et al., 2022).
For the relationship between stress and suicidal risk, the stress of the sample group was significantly positively associated with suicidal risk at a moderate level (r = 0.305, p <0.01). This finding of a positive correlation between stress and suicidal risk may be due to the study’s cross-sectional research design. It was conducted during a time when the Thais who participated in the present study experienced stressful events, such as being laid off and tried to cope with these for a period of time. In other words, their moderate stress was caused by stressors. However, stress caused by the anticipation of loss or harm can lead to difficulties and problems, such as life insecurity, fear, anxiety, anger, and depression, which can be life-threatening. Without adequate treatment or alleviation, depression can trigger suicidal thoughts and behaviors (Briere et al., 2019). This is consistent with the results of the study conducted by Simsir et al. (2022) found that fear of COVID-19 was associated with anxiety (r = 0.55), traumatic stress (r = 0.54), distress (r = 0.53), moderate stress (r = 0.47), depression (r = 0.38), and insomnia (r = 0.27).
The stress-coping behaviors of the participants in the present study were significantly positively correlated with suicidal risk at a low level (r = 0.246, p <0.01). This may be due to the secondary appraisal during the COVID-19 pandemic based on experiences, thoughts, and intelligence to deal with what was considered harm, loss, and threat (Suksatan et al., 2021). The participants’ situation could be regarded as a life crisis involving unemployment or loss of income to support themselves and their families. If one automatically develops a negative attitude toward this situation, depression will set in, with a feeling of discouragement, despair, and hopelessness (Simsir et al., 2022). Once these feelings become overwhelming after individuals assess their situation as life-threatening and struggle to cope with their stress as much as possible, but to no avail, they could develop suicidal thoughts and attempt to end their lives, thinking that this is the only solution to their problem (Briere et al., 2019). This is consistent with the results of the study by Kudinova et al. (2022) found that problem confrontation was associated with higher-level suicidal thoughts in youth admitted to a psychiatric hospital. Therefore, health personnel must regularly and thoroughly assess the problems of their patients who have become unemployed due to the COVID-19 pandemic so that they can help these patients adopt proper stress-coping behaviors, which can reduce their suicidal risk. This will lead to the wellness of the unemployed in crises worldwide.
Implications for Nursing Practice
The COVID-19 pandemic underscores the need to implement strategies to protect the mental health of unemployed Thai people. The results of the present study can be made the basis of the development of guidelines for promoting mental health and improving quality of life. They will also help find at-risk individuals and plan their treatment, design activities for reducing such individuals’ stress, and promote appropriate stress-coping behaviors among them. Nurses should screen patients for psychological problems and suicidal risk. In addition, organizing interventions to reduce stress and encourage appropriate stress-coping behaviors is essential, especially for people who have become unemployed during the COVID-19 pandemic.
Strengths and Limitations of the Study
The present study has both strengths and limitations. To the best of our knowledge, it is the first study in Thailand to determine the relationships between stress, stress-coping behaviors, and suicidal risk among the unemployed in Thailand due to the COVID-19 pandemic. Nonetheless, this study also has some limitations. First, it was a cross-sectional study based solely on self-assessment. Second, the sample was drawn from a single macroregion, making it impossible to extrapolate the findings to the entire Thai population. Third, the present study was also conducted in a single Thai province; thus, although this province has a high rate of suicide attempts, the generalizability of the findings is limited. Despite these limitations, we hope that our research will contribute to a better understanding of how Thais who had become unemployed during the COVID-19 pandemic have dealt with stress.
Conclusion
The results of the present study showed that the unemployed, due to the COVID-19 pandemic, had moderate stress levels, moderate stress-coping behaviors (particularly problem alleviation and problem confrontation rather than emotional management), and a high suicidal risk rate (10.07%). Suicidal risk varies with the levels of stress and stress-coping behaviors. Hence, health personnel must regularly and thoroughly assess their patients who have become unemployed due to the COVID-19 pandemic for mental health problems to promote proper stress-coping behaviors and reduce their suicidal risk.