









Background
Hip fractures continue to pose a significant global health concern, particularly among older adults. The aging demographic has led to a potential increase in the number of patients suffering from hip fractures (Kanis et al., 2012; Sucharitpongpan et al., 2019; Wongtriratanachai et al., 2013). Notably, in Thailand, there has been a steady annual rise of 2% in the incidence rate of fractured hips. According to projections by Wongtriratanachai et al. (2013), the number of patients with hip fractures in Thailand may increase from 181.0 per 100,000 in 2006 to 264.6 per 100,000 in 2025 and to 436.1 per 100,000 in 2050.
Following a hip fracture, a significant proportion of patients, ranging from 82% to 90%, require hospitalization for surgery with the primary aim of restoring their mobility status or achieving rapid post-operative mobilization (Sucharitpongpan et al., 2019). However, despite surgical interventions, evidence indicates that individuals with hip fractures often experience a decline in mobility. Research conducted by Steihaug et al. (2018) revealed that many patients encountered impaired mobility, with over 50% of hip fracture patients failing to regain their pre-fracture mobility levels (Hansson et al., 2015; Vochteloo et al., 2013).
Even after being discharged from the hospital, most patients, as reported by Zaslavsky et al. (2015), did not experience significant improvement in their mobility. Many had to rely on walking aids, some could only sit on the bed, others became bedridden, and a few even had to be transferred to nursing homes (Münter et al., 2018). This impaired mobility can have far-reaching consequences, leading to decreased self-reliance, limited physical functioning, an increased risk of injuries, frequent hospitalizations, and even higher mortality rates (Dyer et al., 2016; Jennison & Yarlagadda, 2019).
Mobility decline emerged as a prevalent nursing diagnosis observed in the majority of patients, and it held significant importance in nursing care. Recognizing the potential negative consequences associated with impaired mobility, it became essential for nurses to comprehend the concept of mobility and the various factors influencing it. From the first day post-surgery until the patients’ discharge, nursing efforts played a crucial role, such as early ambulation, implementing fall prevention strategies, and encouraging patients to engage in activities like re-positioning, bed and chair transfers, standing, and walking (Thai Orthopaedic Nurses Society, 2018). By providing such comprehensive care, nurses could contribute to the recovery of their patients’ former mobility levels.
Mobility in patients after hip fracture surgery is influenced by various factors, as revealed by Gonzalez Zabaleta et al. (2016), Ariza-Vega et al. (2017), Mueller-Schotte et al. (2016), and Promchat et al. (2015). These studies highlighted the impact of comorbidity, cognitive function, social support, fatigue, and sleep quality on mobility. However, there is limited research on mobility and its influencing factors, specifically in patients undergoing hip fracture surgery in Thailand. Only a few studies have focused on this aspect, and the findings have been concerning. For instance, Roobsoong et al. (2020) reported that the walking ability of patients after hip fracture surgery was lower than their pre-hip fracture levels, with only 17.3% being able to walk independently one year after surgery (Pipatyaokul, 2017). Similarly, another study found that one year after surgery, only 26.5% of patients could return to their pre-fracture level of mobility (Adulkasem et al., 2021).
Furthermore, the existing studies have only explored bidirectional associations between these influencing factors and mobility without simultaneously examining their combined effects on a specified outcome. Thus, our current study aimed to address this gap by describing mobility and identifying the factors influencing mobility in patients after hip fracture surgery. The findings from our research would be invaluable in developing nursing strategies to enhance mobility and improve the quality of care for patients with fractured hips.
Our study was guided by the Theory of Unpleasant Symptoms of Lenz and Pugh (2014), which consists of three main elements: symptom experience, influencing factors, and performances. Symptom experience in this context emphasizes the subjective perception of symptoms rather than just objective observation of signs. Previous research has indicated that hip fracture patients often experience pain, which can significantly impact their ability to walk. Gheorghita et al. (2018) found that pain in these patients was associated with a reduced tolerance for walking. Münter et al. (2018) also observed that patients with fractured hips may suffer limited movement and mobility due to pain. Furthermore, Salpakoski et al. (2010) conducted a cross-sectional study revealing that patients with severe pain had a higher risk of experiencing a decline in mobility compared to those with less or no pain (OR = 3.5, p <0.05). Moreover, Foss et al. (2009) discovered a significantly negative correlation between functional mobility and pain related to hip flexion (r = -0.43, p <0.001) as well as pain during walking (r = -0.36, p <0.01).
Patients who have undergone hip fracture surgery commonly experience sleep problems, as evidenced by various studies. Approximately 36% of these patients reported having sleeping difficulties (Cho et al., 2020). Furthermore, a significant number, 78% of patients, had abnormal sleep durations (Kuo et al., 2016). On average, patients experienced 5.4 hours of sleep per night, with around 5.3 awakenings (Reppas Rindlisbacher et al., 2021).
Moreover, the duration of sleep has been found to have an impact on mobility. Patients who slept for 9 hours or more had a decline in walking speed (p <0.05). On the other hand, those with sleep durations of ≤6 hours were associated with increased mobility limitations (OR = 3.62, 95% CI = 1.40–9.37). Poor sleep quality can lead to nocturnal arterial oxygen saturation, which, in turn, affects balance and contributes to mobility limitations (Stenholm et al., 2010).
Between 20% to 40% of patients who undergo hip fracture surgery experience fatigue, often caused by factors such as blood loss, poor nutrition, and low hemoglobin levels. Fatigue is a major hindrance for patients in achieving independent mobility after surgery, accounting for more than 85% of cases where patients struggle to regain mobility (Münter et al., 2018). Even during rehabilitation, fatigue remains a significant problem for hip fracture patients, particularly when they return home after surgery. A study by Mueller-Schotte et al. (2016) revealed that fatigue was associated with lower mobility in these patients compared to non-fatigued individuals.
The Theory of Unpleasant Symptoms (TOUS) focuses on three main influencing factors: physiological, psychological, and situational. Comorbidity, as a physiological factor, can impact the brain and nervous system, leading to impaired mobility (King et al., 2014). Moreover, the greater the number of comorbidities, the more pronounced the impact on mobility (Tam et al., 2020). Cognitive function, as a psychological factor, is significantly correlated with mobility (Ariza-Vega et al., 2017; Lenze et al., 2004), with studies indicating that impaired cognition may lead to reduced mobility potential compared to individuals without cognitive impairment (Münter et al., 2018). Social support, as a situational factor, has been shown to predict walking and stair-climbing abilities (Shyu et al., 2010), and low social support is associated with mobility decline (Nuotio & Luukkaala, 2016).
Based on these factors, it was hypothesized that comorbidity, cognitive function, social support, fatigue, sleep quality, and pain collectively influence the mobility outcomes of patients after hip fracture surgery. Understanding the interactions between these factors will contribute to improving the management and care, ultimately enhancing their post-surgery mobility and overall recovery.
Methods
Study Design
A cross-sectional study design was employed, and the study reporting adhered to the STROBE (Strengthening the Reporting of Observational Studies in Epidemiology) guidelines for cross-sectional studies as proposed by Von Elm et al. (2007).
Samples/Participants
G*Power 3.1 was utilized to calculate sample size in this study, with a power of test set at 0.80, an alpha value of 0.05, and an effect size of 0.10, which was based on the effect size reported in a previous study (Mariconda et al., 2016). Considering six independent variables, the calculated total sample size for the study was determined to be 143 participants. To achieve this sample size, a multi-stage random sampling technique was employed (LoBiondo-Wood & Haber, 2014). Firstly, three health regions were randomly selected out of the 13 regions across Thailand. Next, hospitals were categorized into three levels - advanced-level hospitals (A-level), standard-level hospitals (S-level), and middle1-level hospitals (M1-level). Each hospital level was then randomly assigned to each of the selected health regions. Subsequently, one hospital was randomly chosen from each health region. The sample size of each hospital was proportionally determined based on the total number of patients in that setting. In the final stage, potential participants were recruited using a systematic random sampling approach. Every 3rd patient in the hospital’s patient population was selected to be part of the study. Participants had to meet specific inclusion criteria, which included being aged 50 and older, having a hip fracture resulting from low-energy trauma, having undergone hip fracture surgery, and being able to communicate in Thai. Those experiencing myocardial infarction, severe psychotic disorder, and high blood pressure, and those unable to walk before the fractured hip were excluded from the study.
Instruments
Permission from the original developers was sought before using the questionnaires. Two questionnaires, the de Morton Mobility Index (DEMMI) and the Groningen Orthopedic Social Support Scale (GOSSS), were translated from English into Thai by the primary investigator (PI) using the forward-back translation method as described by Sperber et al. (1994). To ensure content validity, all instruments were validated by five experts, comprising one physician who specialized in orthopedic surgery, two nursing professors with expertise in medical-surgical nursing (orthopedics) and adult-gerontological nursing (orthopedics), as well as two advanced practice nurses (APNs) in orthopedics. Following this validation process, the instruments were tested for reliability in a separate group of 30 Thai patients who shared similar characteristics with the main participants but were not part of the primary study. The instruments used in this study were described as follows:
Demographic and Illness Data Form
This form was used to collect information on various aspects of the participants, including participants’ gender, age, marital status, education, income, living arrangement, number of family members, family history of hip fracture, smoking status, and alcohol consumption. Furthermore, the form also gathered illness-related history, consisting of questions about family history of hip fracture, cause of the fracture, fracture type, and details of the operation. In addition, relevant clinical data were extracted from the participants’ medical charts.
De Morton Mobility Index (DEMMI)
It consisted of a 15-item scale, where eleven items were scored either 0 or 1, and four items were scored 0, 1, or 2. The total score, referred to as the raw ordinal DEMMI score, ranged from 0 to 19. However, using a conversion table, the raw DEMMI score was transformed into an interval-level DEMMI score ranging from 0 to 100. A higher score on the interval-level DEMMI indicated better mobility. It is worth noting that there was no specific cutoff point for the score. The DEMMI scale demonstrated sound psychometric properties, being reliable and valid for assessing mobility in diverse populations, including patients post-hip fracture surgery (de Morton et al., 2013). In the current study, the inter-rater reliability of the Thai-DEMMI was found to be 0.96, and the internal consistency, as tested by Cronbach’s alpha, was 0.88.
Parker Mobility Scale (PMS)
PMS was used to evaluate levels of mobility. This assessment comprised three inquiries that gauged mobility within distinct scenarios: navigating within one’s residence, egress from the residence, and shopping excursions. Each query was appraised on a scale of 0 to 3, denoting degrees of mobility (0: not at all, 1: with assistance from another person, 2: aided by an assistive device, 3: no difficulty). The cumulative score ranged from 0 to 9, as established by Parker and Palmer (1993). Internal consistency, as determined by Cronbach's alpha, yielded a robust value of 0.88. This scale was translated into Thai using the forward-only translation method (Maneesriwongul & Dixon, 2004).
Charlson Comorbidity Index (CCI)
It comprised 21 items representing different comorbidities (Charlson et al., 2008). The total CCI score was obtained by summing up the weights assigned to each comorbidity. A score of zero indicated the absence of comorbidities, while higher scores suggested a greater likelihood of predicted outcomes such as mortality or increased resource utilization. The total CCI scores were categorized as mild (scores of 1-2), moderate (scores of 3-4), and severe (scores ≥5) (Charlson et al., 1987). The Thai version of the CCI was translated into Thai using the International Classification of Diseases codes as a reference (Suwanno et al., 2009). The CCI had sound psychometric properties, including predictive, concurrent, and incremental validity. Additionally, it showed good inter-rater reliability, which was confirmed in the current study with an inter-rater reliability of 0.96.
General Practitioner Assessment of Cognition (GPCOG)
It was utilized to measure cognitive function (Brodaty et al., 2002). It consisted of nine items for patients and six items for an informant. Higher scores on the GPCOG indicated better cognitive function. However, it should be noted that low scores might be influenced by factors such as effort, language barriers, or fatigue. The GPCOG Thai version was translated into Thai using the forward-back translation method described by Griffiths et al. (2015). In the current study, the reliability of the GPCOG was tested using the KR-20 coefficient, which resulted in a value of 0.86.
Groningen Orthopedic Social Support Scale (GOSSS)
The GOSSS was used to assess social support. It consisted of twelve items, which were rated on a 4-point Likert scale, ranging from one (“never or rarely”) to four (“often”). The total score could range from 0 to 48, with higher scores indicating higher levels of social support. Regarding psychometric properties, the internal consistency of the GOSSS was sound. Van Den Akker-Scheek et al. (2004) also conducted a factor analysis on the GOSSS, revealing two factors: perceived social support and instrumental support. Regarding the reliability of the current study, Cronbach’s alpha was used, resulting in a coefficient of 0.85.
Fatigue Severity Scale (FSS)
It was used to assess fatigue severity in the study. It consisted of nine items, each rated on a 7-point Likert scale, ranging from one (strongly disagree) to seven (strongly agree). The total possible scores on the FSS ranged from 9 to 63, with higher scores indicating higher levels of fatigue severity. The cutoff point for indicating the presence of fatigue on the scale was set at ≥4 (Krupp et al., 1989). For the Thai version of the FSS, Sawasdee et al. (2017) translated the scale using the forward-only translation method. The reliability of the FSS was tested in the current study using Cronbach’s alpha, resulting in a coefficient of 0.82.
Pittsburgh Sleep Quality Index (PSQI)
It was used to evaluate the quality of sleep in the study. The Thai version of the PSQI was translated using the forward-backward translation methods by Jirapramukpitak and Tanchaiswad (1997). The PSQI consisted of several components, including the duration of sleep, disturbance during sleep, sleep latency, daytime dysfunction due to sleepiness, sleep efficiency, overall sleep quality, and the use of sleep medications. Scores from each component were added together to obtain a total score. A higher total score indicated poorer sleep quality. The cutoff point for identifying poor sleep quality on the PSQI was set at ≥5 (Buysse et al., 1989). The reliability of the PSQI was assessed in this study using Cronbach’s alpha, resulting in a coefficient of 0.82.
Numeric Pain Rating Scale (NPRS)
It was used to measure pain intensity in the study. This numeric scale ranged from “0,” indicating “no pain,” to “10,” representing the “worst pain imaginable.” Higher scores on the NPRS indicated greater pain severity (McCaffery & Pasero, 1999). The test-retest reliability of the NPRS was assessed in the current study and resulted in a coefficient of 0.89.
Data Collection
Data were collected between August 2022 and February 2023. To initiate the study, an official letter was sent from the Nursing Faculty at Chulalongkorn University to the hospital directors and head nurses of the hospitals where the research was conducted. The investigators then explained the study’s purpose and methodology to potential participants. Informed consent was obtained from each participant before the data collection. The data gathering and mobility assessments were conducted in a prepared and quiet room, and each participant took approximately 30 to 45 minutes to complete.
Data Analysis
SPSS version 26.0 was employed for data analysis. Descriptive statistics were computed for quantitative variables such as age, weight, height, and body mass index (BMI). Multiple linear regression with the enter method was used to examine the relationships between the variables. A significance level of alpha <0.05 was considered to determine statistical significance. Prior to analysis, assumptions of multiple regression were checked to ensure the validity of the results. These assumptions included normality, linearity, heteroscedasticity, independence of error terms, and multicollinearity (Tabachnick & Fidell, 2013). The data was found to have no missing values or outliers. Cook’s distance, a measure of influence on regression estimates, ranged from 0.000 to 0.096, and no case had an outlier value exceeding 1.00. These findings indicate that the data met the necessary assumptions, ensuring the reliability of the regression analysis.
It is noteworthy that mobility assessment in this study used both DEMMI and PMS instruments. However, solely data from DEMMI was employed for regression analysis purposes, whereas data from PMS was exclusively utilized for descriptive purposes.
Ethical Considerations
The Ethics Review Committee of Chulalongkorn University approved the study with COA No. 137/65 in June 2022. Before enrolling in the current study, all participants provided their informed consent by signing consent forms.
Results
Description of the Participants
The study achieved a response rate of 100% from the participants. The results revealed that the mean age of the participants was 74.57 (SD = 10.00). The majority of the participants were female (76.2%), married (80.4%), unemployed (86.7%), and had education at or below the bachelor’s level (74.8%). Almost all of them lived in extended families (97.9%) and identified as Buddhist (99.3%) (Table 1).
| Characteristics | n | % | Mean (SD), Min - Max |
|---|---|---|---|
| Age (years) | |||
| 50-59 (adult) | 15 | 10.5 | 74.57 (10.00), 52-97 |
| 60-69 (young-old) | 31 | 21.7 | |
| 70-79 (middle-old) | 42 | 29.3 | |
| 80 and older (oldest-old) | 55 | 38.5 | |
| Gender | |||
| Male | 34 | 23.8 | |
| Female | 109 | 76.2 | |
| Marital Status | |||
| Single | 28 | 19.6 | |
| Married | 115 | 80.4 | |
| Education | |||
| No education | 21 | 14.7 | |
| lower or equal to bachelor degree | 107 | 74.8 | |
| higher than bachelor degree | 15 | 10.5 | |
| Living Condition | |||
| With family members | 140 | 97.9 | |
| With significant others (not family members) | 3 | 2.1 |
As seen in Table 2, the patients’ BMIs had a mean of 22.1 kg/m2 (SD = 3.8). The average time after surgery was 6.66 months (SD = 3.45). In terms of fracture types, intracapsular hip fractures were the most common (55.9%). Approximately 59.4% of patients underwent arthroplasty as a treatment for their hip fractures. Regarding the causes of hip fractures, falls accounted for the majority (91%). Among the fall-related cases, slipping was the leading cause, contributing to 49.7% of the fractures. The average length of stay in the hospital was 8.80 days (SD = 3.58).
| Clinical Characteristics | n | % | Mean (SD), Min - Max |
|---|---|---|---|
| BMI (kg/m2) | |||
| <18.5 (Underweight) | 22 | 15.4 | 22.10 (3.80), 14.29 - 32.87 |
| 18.5-24.9 (Healthy weight) | 90 | 62.9 | |
| 25 - 29.9 (Overweight) | 28 | 19.6 | |
| ≥30 (Obese) | 3 | 2.1 | |
| Types of Fracture | |||
| Neck femur fracture | 80 | 55.9 | |
| Intertrochanteric fracture | 62 | 43.4 | |
| Subtrochanteric fracture | 1 | 0.7 | |
| Types of Orthopedic Surgery | |||
| Total hip arthroplasty | 21 | 14.7 | |
| Hemi hip arthroplasty | 64 | 44.7 | |
| Internal fixation | 58 | 40.6 | |
| Causes of Hip Fractures | |||
| Fall | |||
| Slipping | 71 | 49.7 | |
| Tripping | 42 | 29.4 | |
| Fall from chair/bed | 10 | 7.0 | |
| Loss of balance | 4 | 2.8 | |
| Being attacked by a person/dog | 3 | 2.1 | |
| Fainting | 6 | 4.2 | |
| Leg weakness | 7 | 4.8 | |
| Length of Stay (days) | |||
| 1-7 days | 58 | 40.6 | 8.80 (3.58), 3-26 |
| 8-14 days | 73 | 51 | |
| 15-30 days | 12 | 8.4 |
Note. BMI (kg/m2) according to World Health Organization (2023)
Description of Mobility Measured at 2 Points of Time (Pre-Hip and Post-Hip Fracture Surgery) using PMS
According to Figure 1, after hip fracture surgery, the percentage of participants who were able to walk during shopping decreased to 25.2% (compared to 71.3% before the fracture). Additionally, the percentage of participants who were able to walk outdoors also reduced to 21.7% (compared to 22.4% before the fracture). In contrast, the percentage of participants who were able to walk only indoors increased to 53.1% (compared to 6.3% before the fracture).
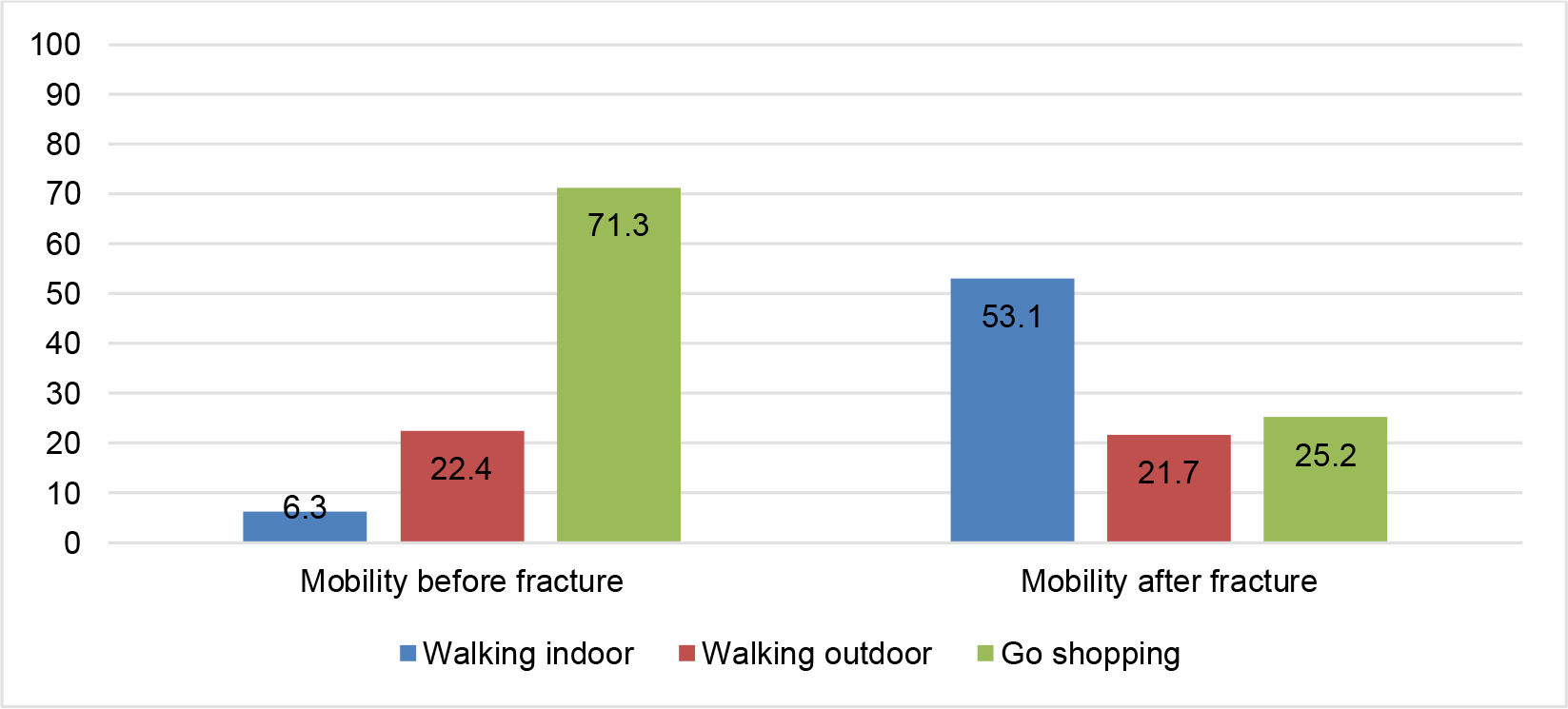
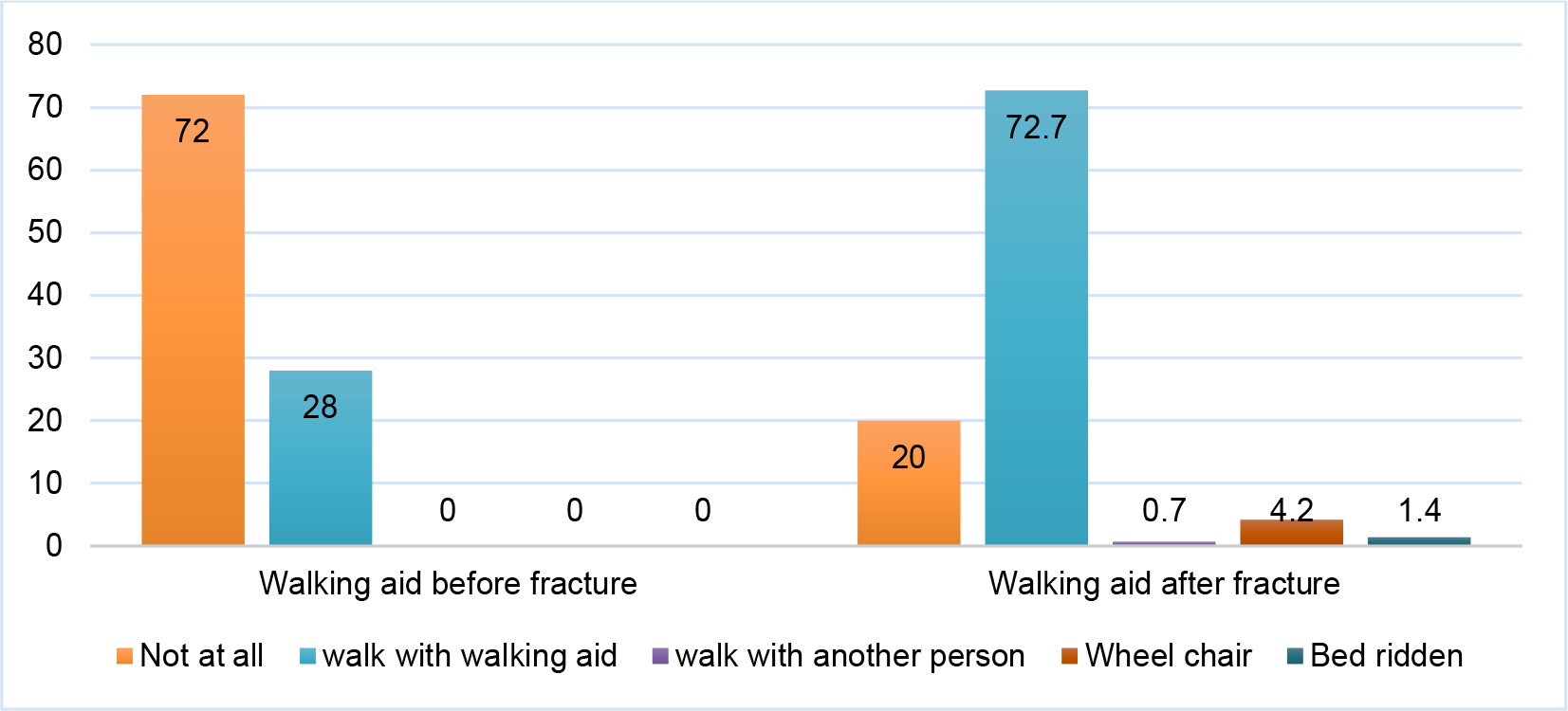
Figure 2 illustrates the changes in participants’ mobility before and after hip fracture. Before the hip fracture, 72.0% of the participants could walk independently without aids. However, after hip fracture surgery, this percentage dropped to 20.0%. On the other hand, the percentage of participants who required walking aids increased from 28.0% before the fracture to 72.7% after surgery. Furthermore, after surgery, 4.2% of participants relied on a wheelchair for mobility, and 1.4% were bedridden.
Description of Mobility Measured by the DEMMI
The mean total raw score for DEMMI was 11.25 (SD = 4.40), whereas the mean converted DEMMI score was 48.86 (SD = 17.89). Scores ranged from 0 to 19 for the total raw score and 8 to 85 for the converted score. Different mobility categories had specific mean scores and standard deviations (Table 3).
| Mobility | Possible Range | Actual Range | Mean | SD |
|---|---|---|---|---|
| Bed (3 items) | 0-4 | 1-4 | 3.69 | 0.63 |
| Chair (3 items) | 0-4 | 0-4 | 2.94 | 0.95 |
| Static balance (4 items) | 0-4 | 0-4 | 1.74 | 1.18 |
| Walking (2 items) | 0-4 | 0-4 | 2.03 | 1.36 |
| Dynamic balance (3 items) | 0-3 | 0-3 | 0.85 | 0.93 |
| Total raw score of patients | 0-19 | 1-18 | 11.25 | 4.40 |
| DEMMI score (converted) | 0-100 | 8-85 | 48.86 | 17.89 |
Description of Influencing Factors of Mobility
Regarding participants’ comorbidities, the mean CCI score was 2.14 (SD = 1.76), and 80.4% had comorbidities. Concerning cognitive function, the majority of participants (85.3%) experienced cognitive problems, with 37.8% having a cognitive impairment and 47.5% experiencing mild cognitive impairment. Regarding social support, participants reported good support, with a mean GOSSS score of 39.2 (SD = 4.91). As for unpleasant symptoms, such as pain, 47.5% of participants experienced mild pain, 32.2% perceived pain at a moderate level, and 1.4% reported pain as “worst pain”. Nearly half of the participants (46.9%) reported experiencing “fatigue,” with an FSS score ≥4. Furthermore, 88.8% of participants complained about “poor sleep quality,” with a mean PSQI score equal to 10.15 (SD = 4.49) (Table 4).
| Variables | n | % | Mean (SD), Min - Max |
|---|---|---|---|
| Comorbidity | |||
| No comorbidity (0 score) | 28 | 19.5 | 2.14 (1.76), 0-6 |
| Low comorbidity (1-2 score) | 67 | 46.9 | |
| Moderate comorbidity (3-4 score) | 31 | 21.7 | |
| High comorbidity (5 score) | 17 | 11.9 | |
| GPCOG | |||
| Cognitive impairment (0 to 4 scores) | 54 | 37.8 | 5.55 (2.46), 1-9 |
| Mild cognitive impairment (5 to 8 scores) | 68 | 47.5 | |
| No cognitive impairment (9 scores) | 21 | 14.7 | |
| Pain | |||
| No pain (0) | 27 | 18.9 | 2.66 (1.84), 0-7 |
| Mild level (1-3) | 68 | 47.5 | |
| Moderate level (4-6) | 46 | 32.2 | |
| Severe level (7-10) | 2 | 1.4 | |
| Fatigue | |||
| FSS score <4 (no fatigue) | 76 | 53.1 | 3.75 (1.18), 1-7 |
| FSS score ≥4 (fatigue) | 67 | 46.9 | |
| Sleep | |||
| PSQI score <5 | 16 | 11.2 | 10.15 (4.49), 2-20 |
| PSQI score ≥5 | 127 | 88.8 |
Regression Analysis of Factors Influencing Mobility
The analysis showed that a combination of comorbidity, cognitive function, social support, pain, fatigue, and sleep jointly accounted for 61.8% of the variance in mobility among the participants (R2 = 0.618; F = 36.598; p <0.001). This suggests that these factors have the potential to predict the participants’ mobility outcomes (Table 5).
| Model | Unstandardized Coefficients | Standardized Coefficients | t | p-value | |
|---|---|---|---|---|---|
| B | Standard Error | Beta | |||
| (Constant) | 44.619 | 9.411 | 4.741 | <0.001 | |
| Comorbidity | -1.591 | 0.597 | -0.156 | -2.664 | 0.009 |
| Cognitive function | 2.258 | 0.436 | 0.310 | 5.178 | <0.001 |
| Social support | 0.527 | 0.201 | 0.145 | 2.616 | 0.010 |
| Pain | -1.708 | 0.576 | -0.176 | -2.964 | 0.004 |
| Fatigue | -0.419 | 0.112 | -0.249 | -3.746 | <0.001 |
| Sleep | -0.673 | 0.255 | -0.169 | -2.644 | 0.009 |
| R2 = 0.618, F = 36.598, df = 6, 136, p <0.001, adjust R2 = 0.601 | |||||
Discussion
The findings revealed that the mobility in patients after hip fracture surgery significantly declined compared to their pre-fracture state, as measured by the PMS. Before the hip fracture, 70% of the patients were able to walk independently, but after the surgery, only 21% retained this ability without using walking aids. These findings are consistent with a previous study conducted by Hao et al. (2020), where it was observed that approximately one month after surgery, only 16% of hip fracture patients could walk independently. Around 54% of the patients required walking aids and assistance, 23% were unable to walk, and 7% were bedridden or unable to move.
Furthermore, when mobility was assessed using the DEMMI, the scores obtained in the current study were notably low, with a mean score of 48.86 on a scale of 0-100. A similar observation was made by Rosendahl-Riise et al. (2020) in their research on patients post-hip fracture surgery, where mobility scores were also found to be low. This suggests that after surgery, most fractured hip patients experienced a significant decline in their mobility levels, losing at least one level of their previous mobility ability.
Factors influencing mobility were identified in the current study. Comorbidity was found to be a significant influencing factor in mobility. Similarly, Gonzalez Zabaleta et al. (2016) conducted a prospective study and reported comorbidity as a predicting factor of mobility (OR = 1.407, p <0.05). Tam et al. (2020) also observed that for every 1 unit increase in comorbidity score, the likelihood of walking independently decreased by 33%.
Pain, especially hip fracture-related pain, was another influencing factor of mobility in the current study. Foss et al. (2009) emphasized that patients experiencing pain were at greater physical risk, leading to limited function ability, reduced walking distance, and level of function. Kristensen (2013) mentioned that some patients experienced pain during rehabilitation while sitting or walking, which could be a result of tissue damage around the prosthesis or surgical site, especially in trochanteric fractures, and loss of knee-extension strength after surgery.
Our study also identified cognitive function as an influencing factor in mobility. Tam et al. (2020) highlighted that poor cognitive function could be a barrier to rehabilitation and hinder the completion of physiotherapy. Ariza-Vega et al. (2017) reported that cognitive function was one of the factors influencing post-operative mobility among patients after hip fracture. Mariconda et al. (2016) indicated that cognitive scores significantly influenced mobility (R2 3-5%, p <0.001).
Social support emerged as another factor influencing mobility, consistent with previous studies. Nuotio and Luukkaala (2016) and Levasseur et al. (2015) also found that social support positively influenced mobility. In Thai culture, filial piety and family support are crucial in encouraging patients’ participation in rehabilitation (Tan et al., 2011). High social support enhances post-operative recovery and achieving recovery goals (Stott-Eveneshen et al., 2017).
Fatigue was a significant factor affecting mobility. Patients experienced tiredness and exhaustion involving muscle weakness, which affected various physical capacities, including walking and other activities of daily living (Pope, 2020). A significant number of patients reported experiencing fatigue and feeling tired, leading them to take rest for hours (Alsén & Brink, 2013). Mueller-Schotte et al. (2016) observed that patients with fatigue symptoms had impaired mobility compared to non-fatigued individuals.
Finally, sleep also played a role in influencing mobility. Agmon et al. (2016) found that sleep disorders were associated with decreased walking speed and mobility. Sleep problems might increase inflammation and insulin resistance (Van Cauter, 2011). The alterations in immunology, metabolic, and endocrinologic systems, along with the loss of muscle strength caused by sleep problems, directly led to functional decline (Barzilay et al., 2009). Additionally, decreased sleep duration was shown to affect femoral muscle strength after hip fracture, further impacting mobility (Kuo et al., 2016).
Implications of the Study for Nursing Practice and Healthcare Policy
Implications for nursing practice are evident from the study findings. Professional nurses should implement effective interventions to address mobility enhancement, pain management, fatigue management, sleep improvement, patient education, regular assessment, and social support integration. These interventions can potentially modify the influencing factors of mobility in patients after hip fracture surgery. Early rehabilitation is vital for patients with comorbidities and cognitive issues, and regular home visits can provide essential support for successful mobility recovery. In addition, interdisciplinary collaboration is necessary, given the complex nature of factors influencing mobility. Nurses should collaborate with other healthcare professionals, including physical therapists, occupational therapists, and physicians, to develop comprehensive care plans to enhance mobility.
The findings also highlight the need for further studies in this area. While the current study identified important factors influencing mobility, other variables might be yet to be explored. Conducting additional research will deepen our understanding and pave the way for more targeted and effective interventions.
Furthermore, for healthcare policy, this study’s findings emphasize the crucial role of policymakers, particularly the Ministry of Public Health, in shaping healthcare policies and action plans. Policies should take into account variables such as comorbidity, cognitive function, pain, fatigue, and sleep quality to enhance mobility post-hip fracture surgery. By addressing these factors in healthcare policy, healthcare providers can improve patient outcomes and quality of life after hip fracture surgery.
Limitations of the Study
The participants in this study were recruited from the outpatient department, which may have resulted in some frail hip fracture patients not being included in the sample. These patients might have found it inconvenient to visit the hospital for outpatient care. Therefore, when generalizing the study findings, caution should be exercised, as the sample may not fully represent the entire population of hip fracture patients, particularly those who are less likely to access outpatient services.
Conclusion
The study revealed that comorbidity, cognitive function, fatigue, pain, sleep quality, and social support significantly influenced mobility among individuals with fractured hips post-surgery. Future research should focus on testing the effectiveness of interventions and therapies that target and modify social support, pain management, sleep quality, and fatigue in this population. Additionally, conducting research with interdisciplinary health personnel is essential that could lead to improved outcomes, including enhanced mobility, quality of life, and overall health outcomes for these patients.