









Background
Nurses play a crucial role in delivering quality healthcare services to patients (Kaya & Boz, 2019). As part of their professional responsibilities, nurses frequently encounter situations that necessitate the application of ethical principles in their practice. Ethics in nursing aims to minimize harm to patients and uphold their values (Ayla et al., 2018). The nursing profession adheres to five fundamental ethical principles: beneficence, non-maleficence, autonomy, confidentiality, and justice (Varkey, 2021). Previous research has highlighted that ethical dilemmas among hospital nurses often arise from the delicate balance between care and harm, the impact of work overload on quality, and resulting disagreements (Haahr et al., 2020). Nurses are faced with the challenge of evaluating their attitudes and actions to ensure adherence to ethical principles, particularly when interacting with patients, their families, and other healthcare professionals (International Council of Nurses (ICN), 2021). Recognizing ethical challenges and dilemmas and making sound decisions based on personal morals and applicable laws are crucial competencies for nurses (Haddad & Geiger, 2018).
One notable ethical case involves the unauthorized disclosure of a condition of a patient with breast cancer to their fiancé, leading to significant consequences for their decision to marry (Pramono, 2018). Such incidents highlight the ethical importance of protecting patients’ privacy and the need for patients to consent to disclose their health information to family members (Tariq & Hackert, 2018). Moreover, the ongoing pandemic has presented nurses with additional ethical dilemmas, including balancing patient care priorities with their own health needs (Alloubani et al., 2021), indicating the multifaceted nature of ethical decision-making within nursing practice.
Nursing education incorporates ethics-related coursework into the curriculum to equip nurses with ethical competencies. Ethical education in nursing begins early in nursing programs in many countries and should continue throughout nurses’ professional careers (Ayla et al., 2018; Robichaux et al., 2022). However, the absence of explicit nursing ethics content in some curricula has highlighted the need to emphasize ethical nursing education (Robichaux et al., 2022).
Our preliminary study involving 67 Indonesian nursing students in 2022 revealed that 40% believed they could discuss patient cases with their peers, potentially violating patient confidentiality and leading to complaints about information leakage. This finding, along with the case mentioned above, highlights the importance of evaluating the ethical behavior of nurses in protecting patient rights. This assessment can serve as a basis for interventions aimed at enhancing nurses’ ethical conduct. No questionnaire exists that specifically measures the ethical behavior of nurses in Indonesia. This lack of precise measurement risks perpetuating inconsistent ethical standards and potentially undermines Indonesia’s commitment to upholding universally recognized ethical norms.
A questionnaire on patient rights protection for nurses has been published in English in Turkey by Eyuboglu et al. (2022). The instrument consists of 28 questions categorized into five aspects: honoring the patient’s entitlement to information and autonomous choices, delivering equitable care, adhering to the principle of beneficence and non-maleficence, valuing patients’ preferences and ethical standpoints, and safeguarding patient privacy. This questionnaire is favored for its comprehensive coverage in assessing ethical behavior and its five essential dimensions
Although the questionnaire developed by Eyuboglu et al. (2022) reflects the culture and characteristics of Turkish nurses, its applicability in Indonesia necessitates customization to the local culture and circumstances. It is important to note that the local culture plays a significant role in shaping ethical behavior within a nation (Vitolla et al., 2021). As an example, a specific cultural concept in Indonesia, known as “Siri na passe” among the Bugis people, has a profound impact on various daily behaviors, such as diligence, integrity, teamwork, and conscientiousness. Nurses with Bugis heritage tend to strongly adhere to this ethical paradigm (Sidin & Rivai, 2020).
Due to these cultural variations, the Turkish version of the questionnaire may not fully align with the Indonesian context covering many cultures in Indonesia. Thus, our research aimed to examine the psychometric properties of the Indonesian version of the Nurses’ Ethical Behavior in Protecting Patients’ Rights (I-NEBPPR) scale. This initiative is crucial to ensure the assessment tool fits well with Indonesia’s unique culture, ethics, and specific context. It will improve the scale’s usefulness and accuracy in evaluating nurses’ ethical behavior in the Indonesian healthcare system.
Methods
This study consisted of three phases. During Phase I, the original instrument (NEBPPR) developed by Eyuboglu et al. (2022) was translated following the WHODAS 2.0 translation package (World Health Organization (WHO), 2012). In Phase II, each item’s clarity, relevance, and appropriateness were evaluated using content and face validity. Finally, Phase III was conducted to assess the construct validity, convergent validity, discriminant validity, and reliability.
Phase 1. Forward and Backward Translation
The process was initiated with the original author’s permission to adapt the questionnaire into Indonesian and then use it as a patient rights survey for Indonesian nurses. They also expressed a willingness to assist with the adaptation of this questionnaire. This questionnaire has been translated in accordance with the WHODAS 2.0 translation package (World Health Organization (WHO), 2012). Two professional translators and two translators with a nursing background performed the forward and backward translations so that the questionnaire remained within the context of nursing.
Phase 2. Content and Face Validity
Content validity was assessed through a panel of experts consisting of seven nursing lecturers and one nursing ethics assessor who reviewed the translated version of the NEBPPR questionnaire. The expert panel was comprised of seven nurse lecturers with a diverse array of academic specialties. Two panelists are enrolled in doctoral programs and the remaining five hold master’s degrees in nursing. One panelist, in particular, specializes in nursing curriculum development, and one serves as an ethical review board member. The panel employed a standardized set of criteria based on established guidelines for assessing content validity, focusing on each item’s relevance, clarity, and comprehensiveness in the questionnaire.
They were asked to rate the relevance of 28 items on a scale of 1 to 4, ranging from “irrelevant” to “relevant.” This evaluation aimed to achieve semantic, idiomatic, experiential, and conceptual equivalence between the translated questionnaire and its original version. The evaluation of content validity using Aiken’s V values (Aiken, 1985) involved eight experts, resulting in a V table value 0.75. Among the 28 items, 26 had higher Aiken values than the V table, indicating satisfactory content validity. The two items were retained despite achieving scores under the pre-established Aiken’s V threshold (Penfield & Giacobbi, 2004). This decision was based on the consideration that the items are essential for comprehensively capturing and delineating the multifaceted aspects of ethical conduct. It should also be highlighted that the lower scores ascribed to these items by the panel of experts were primarily attributable to the perception that they more appropriately belong to a different factor.
For face validity, three nurses and fourteen clinical nursing students were recruited as respondents. The inclusion of clinical nursing students was based on their practical experience. The participants answered the questionnaire and provided feedback on their understanding of the content. Revisions were made to items 11, 19, 24, and 25 based on the received feedback. For example, item 11 was modified from “…pays more attention to patients” to “…pays more attention,” while item 19 was changed from “…is more likely to cause injury than to provide benefits to patients” to “…Nursing actions that pose a risk to the patient.” The five-point Likert scale utilized in the original questionnaire, with response options of “never,” “rarely,” “sometimes,” “very often,” and “always,” was found to be acceptable, as there were no reports of confusion in interpreting the scale’s meanings.
In the Indonesian version, the response options were accurately translated as “tidak pernah” (never), “jarang” (rarely), “kadang” (sometimes), “sangat sering” (very often), and “selalu” (always), ensuring the scale’s equivalence. The revised questionnaire was reevaluated by the expert panel, who generally approved the changes. The respondents involved in the face validity assessment were not included in the subsequent CFA. This separation was maintained to ensure the methodological rigor and independence of each validation phase.
Phase 3. Construct Validity, Convergent Validity, and Discriminant Validity, and Reliability
For this phase, the expected number of respondents is tenfold the number of items (Tsang et al., 2017). This questionnaire contains 28 items; therefore, a response rate of at least 280 is required. The respondents in this study were nursing professionals from diverse regions across Indonesia, ensuring a wide geographical representation. As for the eligibility criteria, all respondents were required to have at least one year of professional nursing experience, to deliver direct care to patients, and to be willing to participate in the study.
Data were gathered using the SurveyMonkey platform from 29 October to 30 November 2022. The questionnaire was disseminated via multiple channels, including social media platforms frequented by nursing professionals and through direct social networking. To maximize the likelihood of obtaining qualified respondents, the recruitment message explicitly stated the eligibility criteria of respondents. Respondents signed a consent form explaining that their information would be kept confidential and used only for research purposes. Demographic data such as gender, age, work experience, and data from 28 questions were collected. Two hundred eighty-three nurses completed the questionnaire, and all were used for analysis.
The construct validity was assessed using confirmatory factor analysis (CFA). The reliability test measured internal consistency with Cronbach’s alpha and composite reliability. The IBM SPSS statistics version 27.0 (SPSS Inc, an IBM company, Chicago, IL, USA) was used to analyze demographic characteristics, and AMOS 24.0 was used for model fit. The CFA demonstrates satisfactory model-data fit if the Root Mean Square Error of Approximation (RMSEA) below 0.08, the Comparative Fit Index (CFI) and Goodness of Fit Index (GFI) exceeds 0.9, and the ratio of Chi-Square to degrees of freedom (χ2/df) is below 3, all in alignment with the recommended thresholds (Fan et al., 1999; West et al., 2012).
A Cronbach alpha value above 0.7 indicates acceptable internal consistency (Taber, 2018). The convergent validity is represented by an AVE (Average variance extracted), provided that the composite reliability exceeds 0.6; a value below 0.5 for AVE can be deemed acceptable in certain circumstances (Fornell & Larcker, 1981). Discriminant validity was evaluated using the Fornell-Larcker criterion. Fornell-Lacker’s criterion compares the AVE’s square root to the latent construct’s correlation (Hair Jr et al., 2014).
Ethical Considerations
Approval from the Institutional Review Board was secured through the Committee for Research Ethics of the Faculty of Health Sciences, Universitas Jenderal Soedirman, Indonesia, for this study (Approval number: 885/EC/KEPK/X/2022). To secure informed consent, prospective respondents were presented with a digital information sheet outlining the study’s objectives, eligibility criteria, and the rights and responsibilities associated with participation. A clickable ‘Agree’ option was provided. By clicking ‘Agree,’ respondents were taken as having read, understood, and consented to participate in the research. The informed consent procedure emphasized the anonymity and confidentiality safeguards in place, reiterating that participants’ responses would be utilized solely for academic research purposes. Respondents who proceeded to the subsequent page were considered to have granted their informed consent.
Results
Demographic Characteristics of the Participants
The study involved a predominantly female participant group, with 78.4% (n = 222) of the respondents being female. The participants had a mean age of 34.42 years, ranging from 21 to 55. The working experience of the respondents varied from 1 to 35 years, with an average of 11.04 years. The response rate for the study was 100%, indicating a high level of engagement and participation. The number of respondents (283) exceeded the minimum requirement of 260, ensuring a robust sample size for analysis. A comprehensive description of the participants’ characteristics is presented in Table 1.
| Characteristics | n (%) | Mean ± SD |
|---|---|---|
| Gender | ||
| Male | 61 (21.6) | |
| Female | 222 (78.4) | |
| Age (Year) | 34.42 ± 7.95 | |
| 21-25 | 51 (18) | |
| 26-35 | 111 (39.2) | |
| 36-45 | 94 (33.2) | |
| >45 | 27 (9.5) | |
| Work experience (Year) | 11.04 ± 8.09 | |
| 1-5 | 92 (32.5) | |
| 6-10 | 57 (20.1) | |
| 11-20 | 97 (34.3) | |
| 21-30 | 32 (11.3) | |
| >30 | 4 (1.4) | |
Confirmatory Factor Analysis Results
The reflective outer model did not meet the acceptability criteria in the confirmatory factor analysis for five items (1, 6, 14, 20, and 24) (Table 2) due to factor loadings falling below the minimum threshold of 0.4 (Guadagnoli & Velicer, 1988; Stevens & Stevens, 1992). However, as shown in Table 3, 23 items demonstrated loading factors exceeding 0.4. It is noted that Item 11 had the highest loading factor of 0.871, while Item 19 had the lowest loading factor of 0.453.
| Item | NEBPPR | I-NEBPPR | Factor Loading |
|---|---|---|---|
| Item 1 | I make the care-related decision with the patient | Saya membuat keputusan tentang perawatan bersama-sama dengan pasien | 0.378 |
| Item 6 | I think it is not necessary to explain the practices I will perform to the patients who have lost their ability to make decisions (unconscious) |
Saya merasa tidak perlu menjelaskan tindakan keperawatan yang akan saya lakukan kepada pasien yang tidak mampu untuk membuat keputusan (contoh: pasien yang tidak sadar) | 0.198 |
| Item 14 | I am curious about the private lives of patients | Saya ingin tahu dengan kehidupan pribadi pasien | 0.368 |
| Item 20 | I refrain from interfering in a patient's private life without a medical reason | Saya berusaha untuk tidak mencampuri urusan pribadi pasien yang tidak terkait dengan masalah medis | 0.384 |
| Item 24 | I refrain from performing professional practices refused by the patient | Saya berusaha untuk tidak melakukan tindakan keperawatan yang tidak disetujui pasien | 0.288 |
| NEBPPR | I-NEBPPR | |||
|---|---|---|---|---|
| No | Statement | No | Statement | Factor Loading |
| Factor 1. Respect for right to information and decision making | Faktor 1. Menghormati hak untuk mendapatkan informasi dan membuat keputusan | |||
| 2 | I inform the patient before my professional practices | 1 | Saya memberikan informasi kepada pasien sebelum melakukan tindakan keperawatan | 0.681 |
| 3 | I inform the patients about their rights | 2 | Saya memberi tahu pasien tentang hak mereka | 0.621 |
| 4 | I respect the patient's right to know the caregiver and health professional that will provide treatment | 3 | Saya menghormati hak pasien untuk mengetahui siapa saja tenaga kesehatan yang akan memberikan perawatan | 0.595 |
| 5 | I introduce myself to the patient | 4 | Saya memperkenalkan diri kepada pasien | 0.620 |
| 7 | I receive the patient's consent before performing my professional practices | 5 | Saya mendapatkan persetujuan dari pasien sebelum melakukan Tindakan keperawatan | 0.576 |
| 8 | I inform the patient and/or family about the professional practices I will perform for the patient | 6 | Saya memberi tahu pasien dan/atau keluarga tentang tindakan yang akan saya lakukan kepada pasien | 0.583 |
| 9 | I create an opportunity for the patient to take part in care and treatment decisions | 7 | Saya memberi kesempatan kepada pasien untuk berpartisipasi dalam pengambilan keputusan tentang perawatan dan pengobatannya | 0.500 |
| Factor 2. Providing fair care | Faktor 2. Memberikan perawatan yang adil | |||
| 10 | I provide more attentive care for the patients whose socioeconomic levels are higher | 8 | Saya memberikan perhatian lebih kepada pasien yang memiliki tingkat sosial ekonomi yang lebih tinggi | 0.771 |
| 11 | I provide more attentive care for the patients whose beliefs are similar/close to mine | 9 | Saya memberikan perhatian lebih kepada perawatan pasien yang agamanya sama/mirip dengan agama saya | 0.871 |
| 12 | I refrain from providing care for patients whose political opinions are different than mine | 10 | Saya memilih untuk tidak merawat pasien yang aliran politiknya berbeda dengan saya | 0.517 |
| 13 | I give priority to the families of health professionals in my professional practices | 11 | Saya memberikan prioritas dalam merawat anggota keluarga dari tenaga Kesehatan/karyawan tempat saya bekerja | 0.457 |
| 15 | I provide more attentive care for the patients whose values are similar/close to mine | 12 | Saya memberikan perhatian lebih kepada perawatan pasien yang mempunyai nilai sama/mirip dengan nilai-nilai yang saya junjung | 0.719 |
| Factor 3. Providing benefit-not harming | Faktor 3. Memberikan manfaat-tidak merugikan | |||
| 16 | I assess my professional practices in terms of the risk of harming the patients | 13 | Saya mempertimbangkan Tindakan keperawatan yang saya berikan, apakah Tindakan saya dapat membahayakan pasien | 0.558 |
| 17 | I focus on providing benefits to the patient in my professional practices | 14 | Saya mengutamakan kemanfaatan untuk pasien pada tindakan keperawatan yang saya lakukan | 0.541 |
| 18 | I take precautions against situations that may harm the patient | 15 | Saya berhati-hati terhadap situasi-situasi yang dapat membahayakan pasien | 0.642 |
| Item 19 | I refrain from professional practices that have the risk of providing more harm than benefit to the patient | 16 | Saya berusaha untuk tidak melakukan Tindakan keperawatan yang lebih beresiko memberikan bahaya daripada memberikan kemanfaatan untuk pasien | 0.453 |
| Factor 4. Respect for patient values and choices | Faktor 4. Hormati nilai-nilai dan pilihan pasien | |||
| 21 | I respect a patient’s right to select the caregiver and health professional who will provide care and treatment | 17 | Saya menghormati hak pasien untuk memilih tenaga kesehatan yang akan memberikan perawatan dan pengobatan | 0.619 |
| 22 | I perform my professional practices in the framework of respect for the patient’s beliefs | 18 | Saya melakukan tindakan keperawatan dengan tetap menghormati keyakinan pasien | 0.655 |
| 23 | I respect a patient’s right to perform his/her prayers | 19 | Saya menghormati hak pasien untuk melakukan ibadah atau berdoa sesuai agamanya | 0.708 |
| Factor 5. Attention to privacy | Faktor 5. Perhatian untuk privacy | |||
| 25 | I refrain from sharing information related to a patient’s private life with others without medical reason | 20 | Saya berusaha untuk tidak membagi informasi terkait kehidupan pribadi pasien dengan teman sejawat tanpa alasan medis | 0.616 |
| 26 | I refrain from sharing patient information with the people who are not involved in the care and treatment process | 21 | Saya berusaha untuk tidak membagikan informasi tentang pasien kepada orang yang tidak terlibat dalam proses perawatan dan pengobatan pasien | 0.667 |
| 27 | I feel uncomfortable when the patient files are in a public place/open to all | 22 | Saya merasa tidak nyaman saat dokumen catatan keperawatan pasien diperlihatkan kepada orang lain atau khalayak | 0.711 |
| 28 | I receive the patient’s consent to get a practice done/watched on the patient with training purposes | 23 | Saya mendapatkan persetujuan pasien apabila Tindakan keperawatan yang saya lakukan kepada pasien dilakukan atau diperlihatkan kepada orang lain untuk kepentingan training atau Pendidikan | 0.473 |
The CFA results demonstrated satisfactory model-data fit, as shown in Table 4 and Figure 1. The RMSEA value of 0.044 suggested an excellent fit, given that values above 1 are considered inadequate (MacCallum et al., 1996). Moreover, the GFI, CFI, and Incremental Fit Index (IFI) values surpassed 0.9, which indicated a strong fit (Fan et al., 1999). The relative Chi-square value of 1.554 was lower than 3, further supporting the appropriateness of the model fit.
| Absolute fit index | |||||
|---|---|---|---|---|---|
| χ2 | χ2/df | RMSEA | GFI | CFI | IFI |
| 337.170 (p <0.001) | 1.554 (p <0.001) | 0.044 | 0.906 | 0.929 | 0.930 |
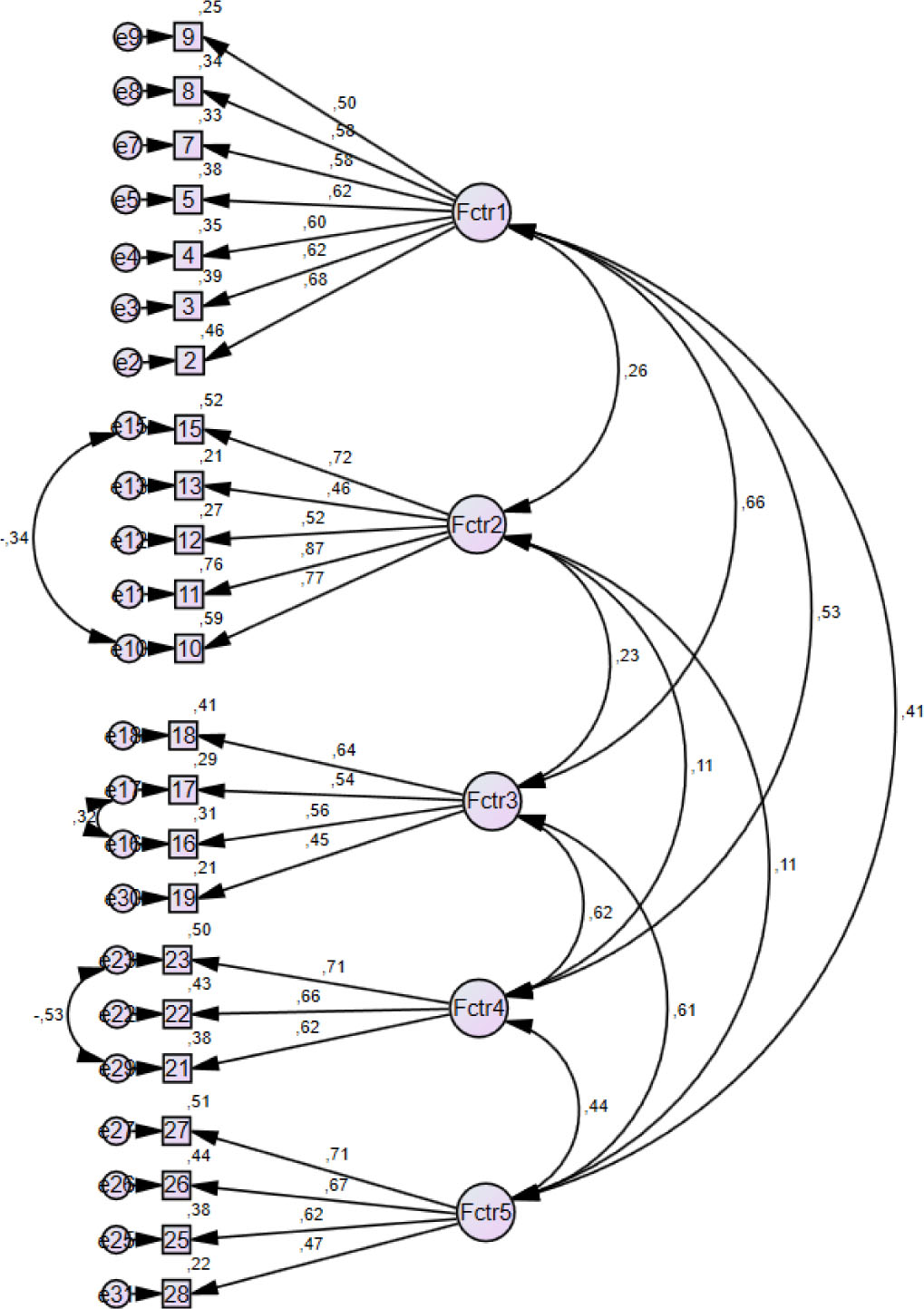
Note: Fctr 1 = Factor 1 (Respect for right to information and decision); Fctr 2 = Factor 2 (Providing fair care); Fctr 3 = Factor 3 (Providing benefit-not harming); Fctr 4 = Factor 4 (Respect for patient values and choices); Fctr 5 = Factor 5 (Attention to privacy)
Reliability, Convergent Validity, and Discriminant Validity
The Cronbach’s alpha value was 0.819, and the composite reliability of all factors was above 0.6, indicating satisfactory reliability and internal consistency. The composite reliability values were greater than 0.6, with Factor 3 having the highest value (0.835) and Factor 2 having the lowest (0.675). The findings demonstrated that the measures employed in the study were dependable. According to the results, Factor 3 had the highest AVE (0.508), while Factor 1 had the lowest AVE (0.358). Furthermore, the square root of AVE in this study was greater than the correlation of latent construct in the same column and row, as shown in Table 5.
| Fornell-Larcker | |||||||
|---|---|---|---|---|---|---|---|
| CR | AVE | 1 | 2 | 3 | 4 | 5 | |
| Factor 1 | 0.795 | 0.358 | 0.599 | ||||
| Factor 2 | 0.675 | 0.469 | 0.217 | 0.685 | |||
| Factor 3 | 0.835 | 0.508 | 0.415 | 0.129 | 0.553 | ||
| Factor 4 | 0.700 | 0.438 | 0.459 | 0.064 | 0.460 | 0.662 | |
| Factor 5 | 0.713 | 0.388 | 0.319 | 0.106 | 0.434 | 0.353 | 0.623 |
Discussion
This research aimed to assess the psychometric properties of the I-NEBPPR. CFA was used to evaluate the construct validity of the I-NEBPPR. The context and culture of the country were considered when adapting a questionnaire (World Health Organization (WHO), 2012; Zahedi et al., 2013), so our evaluation of the targeted questionnaire was based on expert judgment and not simply translation.
Five items (1, 6, 14, 20, and 24) were removed due to relatively low factor loadings. A combination of statistical analysis and considerations of cultural appropriateness within Indonesian nursing guided the removal of specific items from the questionnaire. Item 1, despite its alignment with Indonesian values, was eliminated due to its low factor loading; however, its core concept is adequately captured by Item 2. Item 6, which had the lowest factor loading, was removed; in the context of Indonesian nursing, the notion that patients should be informed about interventions is universally accepted, negating the need for this specific item. Items 14 and 20, which pertain to inappropriate curiosity about a patient’s private life, were also removed; their primary focus is sufficiently represented by Item 15, which evaluates nurses’ respect for patients with differing values. Finally, Item 24 was omitted due to its low factor loading, and its content is already covered by another item in the questionnaire’s fourth domain.
Consequently, the refined questionnaire remains a comprehensive and culturally sensitive instrument for evaluating ethical behavior among nurses in Indonesia. The original questionnaire contains 28 items with factor loadings ranging between 0.40 and 0.81 (Eyuboglu et al., 2022). Similarly, the I-NEBPPR item loading factors range from 0.453 to 0.871. High factor loadings in both questionnaires validate the items attributable to underlying factors. The Cronbach alpha of the original questionnaire was 0.84, whereas, in the current study, it was 0.819. Both internal consistency values are robust (Hinton et al., 2014; Taber, 2018). Internal consistency denotes the extent to which an instrument’s components measure distinct facets of a given attribute or construct (Revicki, 2014). Convergent validity pertains to the degree to which multiple methods measure the same trait (Krabbe, 2017), while discriminant validity refers to the extent to which different traits are distinct from one another (Carmines & Zeller, 1979). In this study, the measured factors demonstrate acceptable convergent validity, as evidenced by the Average Variance Extracted (AVE) values, with Factor 3 displaying the highest AVE (0.508) and Factor 1 showing the lowest AVE (0.358). Based on the Fornell-Larcker criterion, the discriminant validity of the measured constructs can be established. The square root of the AVE values in this study exceeded the correlations observed between the latent constructs in the same column and row. This indicates that the constructs are distinct, supporting their discriminant validity.
The I-NEBPPR questionnaire consists of 23 items, comprising seven items for Respect for the right to information and decision-making, five items for Providing fair care, four items for Providing benefit-not harm, three items for Respect for patient values and choices, and four items for Paying attention to patient privacy. The scores for items in Factor 2 (8, 9, 10, 11, and 12) are reversed. The response options for these items are ordered as “never,” “rarely,” “sometimes,” “very often,” and “always,” respectively, with scores assigned in the opposite direction, ranging from 5 for “never” to 1 for “always.” Therefore, higher scores on these items indicate a lower frequency or occurrence level for the behaviors or characteristics. Based on face and content validity considerations, the original questionnaire’s five-point Likert scale was retained without modification. It was found that the response option “sometimes” did not introduce any ambiguity. The resulting scores ranged from 23 to 115, and the interpretation suggests that higher scores reflect a greater sensitivity to the nurse’s behaviors in protecting patient’s rights (Eyuboglu et al., 2022).
Implications and Limitations
The strengths of this study included the optimal number of respondents based on the number of questionnaire items, ensuring a robust sample size for analysis. Additionally, the utilization of online surveys, known for higher response rates compared to paper-based surveys (Menon & Muraleedharan, 2020), contributed to a remarkable 100% response rate in this study. Another strength was the diverse representation of nurses from various regions in Indonesia, with work experience ranging from one to thirty-five years. This inclusivity allows novice and experienced nurses to benefit from the questionnaire, enhancing its applicability and generalizability. Also, the efficient finalized questionnaire was designed to be completed in less than five minutes. This efficiency enables participants to provide their responses easily and quickly, reducing the burden of participation and enhancing the feasibility of data collection. However, with the newly developed Indonesian version of the questionnaire, improving nursing performance in this area is possible. It is essential to conduct regular assessments of the ethical behavior of nurses, including new nurses, to ensure their adherence to patient rights protection and maintain a high standard of care.
The limitation of this study was its dependence on self-reported information, which could be vulnerable to biases in respondent behavior and the influence of social acceptability. To mitigate the limitations inherent in relying solely on self-reported data, this study recommends incorporating additional observational data to complement the self-reported responses obtained from the questionnaire. This multimodal approach aims to validate the subjective experiences captured in the survey by comparing them with objective observational measurements.
Conclusion
The 23-item I-NEBPPR demonstrated strong psychometric properties, making it a valuable, practical, and time-efficient tool for nurse supervisors, nursing managers, and nursing leaders who evaluate nursing competence and for nursing education institutions in curriculum development. However, it should be noted that the applicability of the I-NEBPPR may be limited to clinical nurses in clinical settings, and using it with nursing students and other healthcare professionals may require further investigation. Future research should explore its application to diverse participant groups. Therefore, it is recommended that nursing supervisors include routine evaluations of nurses' clinically-based ethical behavior using the I-NEBPPR as part of their supervisory responsibilities.